Introduction
According to World Sex Records (1997), “the most orgasms [William Hartman and Marilyn Fithian] recorded in an hour for a woman is a staggering 134, while the best men could do was 16. How we lesser mortals can hope to achieve anything in that vicinity was not discussed” (n.p.). Numerous scholarly articles and blogs/social media/news outlets repeat this data without review or critical thought, despite the lack of published, reliable peer-reviewed data on the so-called record. It is only mentioned by Hartman and Fithian in various interviews. To my knowledge, this is the first review of this apparent record.
Indeed, a woman did ride her bike five miles to Hartman and Fithian’s California-based Center of Marital and Sexual Research in the late 1970s to masturbate. Yet, the claim of 134 orgasms is questionable. Hartman and Fithian’s methodology, relying solely on heart rate in later years—a measure easily influenced by other factors— likely produced this “record” as an artifact. The same is true for the male multiple orgasm record of 16 orgasms in an hour, which was based on the same heartbeat criterion. The researcher’s multiorgasmic typologies—multiorgasmic discrete and multiorgasmic continuous—are descriptions of autonomic dynamics rather than orgasm occurrences. Thus, these typologies should be eliminated in favor of more accurate, less confounding measurements like rhythmic pelvic floor contractions of the urogenital reflex measured by an anal probe with corresponding time-between-evocation nomenclature.
Hartman and Fithian’s Definition of Orgasm
Hartman and Fithian (1984) define orgasm as “a peak in emotional and physical responses, accompanied by pelvic contractions, experienced during sexual stimulation” (p. 4). While they include contractions as part of their definition, they ironically do not use contractions as their orgasm detector, using heartbeat instead. Moreover, they notably diverged from Masters and Johnson’s established sexual response framework by stating they “have not observed the ‘plateau’ phase” (Chalker, 1994, p. 4). During the plateau phase, which precedes orgasm, an individual experiences sustained autonomic arousal characterized by elevated heart rate, muscle tension, and heightened genital sensitivity, but without the distinct neural transition from excitation to inhibition across multiple neural networks in the brain and spinal cord that defines orgasm itself. This departure suggests that they do not seek to distinguish between plateau phase and orgasm. It is likely that they sought to study orgasm, but ended up getting some mix of excitement phase and plateau responses added in with any orgasms due to their use of heartbeat as the only indicator. Although the definition is acceptable, it is unclear whether they actually gathered data on what they sought to research based on this definition.
Summary of Hartman and Fithian Research
A summary of Hartman and Fithian’s research history is provided in Bullough & Bullough’s (1994; 2013) encyclopedia under the “Center for Marital and Sexuality Studies”:
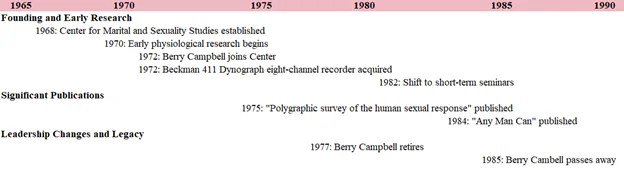
“In 1970, some rudimentary physiological research began. In 1972, the late Berry Campbell, a research physiologist from the University of California Medical School at Irvine, joined the Center quarter-time as part of his teaching load. Campbell initially used borrowed equipment, but the Center itself eventually purchased a Beckman R411 Dynograph eight-channel recorder. To support the research, Hartman and Fithian offered short-term seminars on sexual therapy in most of the major cities in the United States. The first seminar was held for about 20 people, but the numbers built up to as many as 600 in such major centers as New York City. Short-term seminars continued to be held until 1982, and in some years more than two dozen such seminars were held. The money earned from them not only allowed the continuation of the research but also the upgrading and purchase of more and newer research equipment, some made specifically for the Center. Hartman and Fithian not only used the laboratory for their own research, but they allowed a number of other professionals access to it as well” (p. 106).
The timeline below summarizes the research period of Hartman and Fithian.
It is unknown what equipment the researchers obtained besides the recorder:
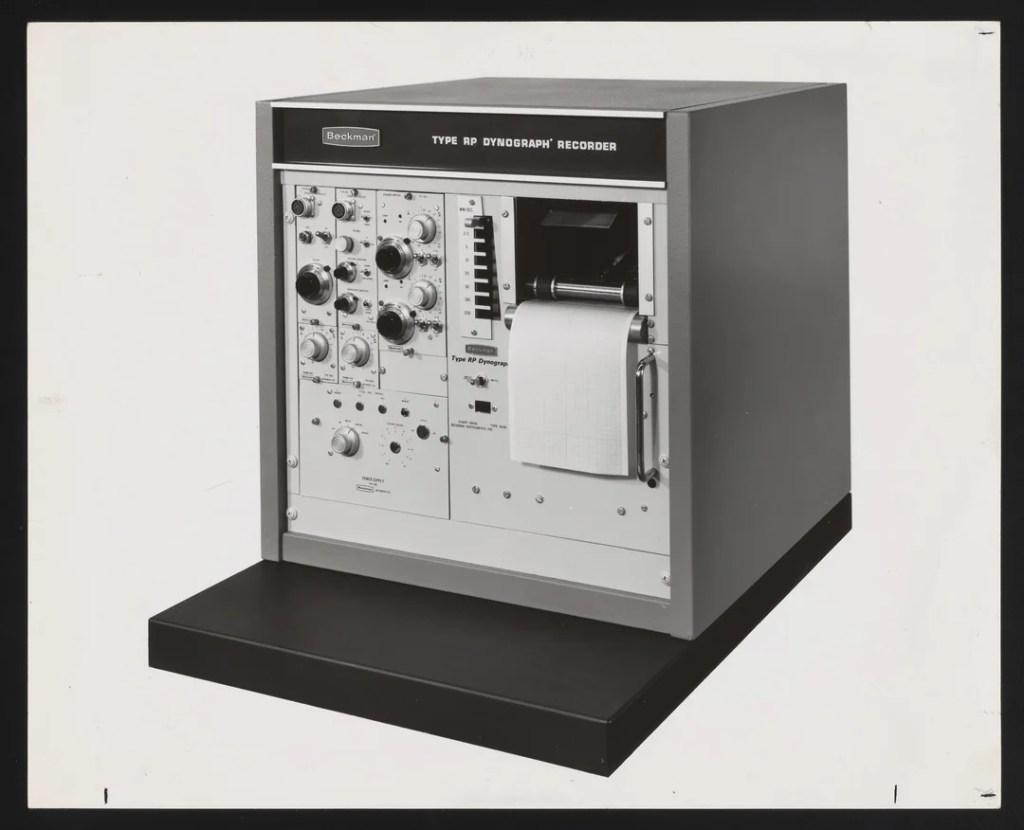
Beckman R411 Dynograph from digital.sciencehistory.org/
The De-evolution of Hartman and Fithian’s Measurement Techniques
Hartman and Fithian were off to a good start with their multi-measurement approach. However, as the 1970s went on, they relied not on self-report, nor EEG, nor respiration, nor gold standard orgasm contractions. They relied on heartbeat, a confounding indicator.
In The Physiologist, Berry Campbell, William Hartman, Marilyn Fithian, and Irene Cambell (1975) describe various measurement techniques that were used without reference to specific Beckman attachment models or other measurement instruments. This would typically be in a methods section, but this abstract appears to be all that was published.
“Information to establish a baseline of human sexual response to serve as a foundation for experimental work was gathered on 23 men and 57 women in 310 polygraphic recordings of 617 orgasms during masturbation and coitus. No critical information of this kind has been amassed before. The events during sexual response have been well described by Masters and Johnson by verbal material does not lend itself to the purposes at hand. We have studied especially vaginal pressure in the different segments of the vagina, rectal pressure, respiratory pattern, ECG, heart rate, and capillary pulse volume. We found that orgasm resulted in simultaneous contraction of all the muscles of the pelvic outlet; thus comparable records could be made from the rectum and vagina, allowing equivalent studies on both men and women and of couples in coitus. Consistency of pattern within the individual and the widest variation between individuals was found. Of the systemic parameters, heart rate only was found to be a reliable indicator of orgasm. What we have called the cardiac crisis is a constant feature of the sexual response. The widespread prevalence of premature ventricular contractions is show. The study suggests that valid experimental series can be set up with a judicious matching of the response patterns” (Campbell, Hartman, Fithian, & Campbell, 1975, p. 159).
As can be taken from this publication, Hartman and Fithian initially employed a multi-modal approach to their research, incorporating rectal probes and other physiological measurements in their early work, but their subsequent methodology took a problematic turn. They are correct that heart rate does become elevated at orgasm relative to baseline, but they abandoned all other ways they originally had to cross-validate the data, such as the gold standard rhythmic contractions of the urogenital reflex. Their determination that heart rate alone served as a reliable indicator of orgasm represents a considerable methodological error, which would later be used as a sole criterion for evidencing orgasm.
In addition, subjective report was allegedly also abandoned by Hartman and Fithian, based on an Anonymous (1997) entry in World Sex Records. It is unknown where this contributor obtained this information.
“For 22 years, Doctors William Hartman and Marilyn Fithian of the Center for Marital and Sexual Studies in Long Beach, California, have been faithfully recording the orgasmic response in their laboratory…. After several false starts (originally they had the subjects push a button whenever they had an orgasm, but during the heat of the moment they usually became too preoccupied to be concerned with the cause of research), the study continued apace, eventually encompassing 751 individuals” (n.p.).
If this is true, the apparent female and male recordholders could have been surprised to hear that they had so many orgasms when the researchers told them what the heart rate data suggested.
Hartman and Fithian’s Heartbeat Method
Hartman and Fithian used peaks of heart rate around 120 beats per minute as evidence that orgasm has occurred. They watch for instances where the heart rate increases, stays at, or fluctuates back and forth around 120 BPM. The absence of any mention of controlling for confounding factors related to heart rate weakens the reliability of their findings. Since there is no scholarly publication reporting the data on these findings, there is both no methods section and no peer review.
Hartman and Fithian (1984, p. 159) do note that anxiety and physical condition can influence heartbeat. Heartrate also can vary based on several factors including:
- Activity level (baseline fitness)
- Level of exertion during masturbation
- Age (maximum heart rate changes)
- Holding the breath
- Cardiac mass/size
- Medical conditions
- Medications
- Time of day
- Position/posture
- Hydration status
- Athletes tend to have lower maximal responses
- Older adults have different ranges
- People with heart conditions have different baselines
- Beta blockers affect maximum heart rate
- Caffeine increases heart rate
Adding to these other factors, the female participant also road her bike 5 miles to get there, which could have increased her baseline! She could have already elevated her heartrate from the start! It is never said the time it took between when she got off the bike and when she did the study.
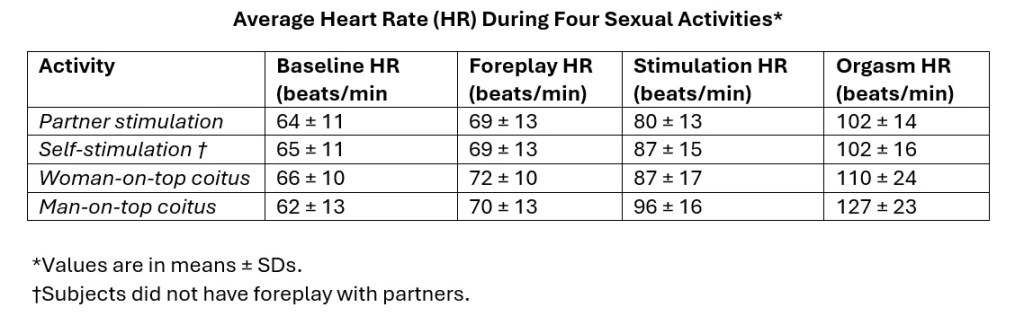
The confounding factors lead the authors to commit a causal attribution fallacy. The same heart rate can come from many different causes, not just orgasm. What counts as “elevated” heart rate varies by individual, and the 120 BPM threshold is arbitrary. Hartman and Fithian can’t reliably work backwards from heart rate to determine cause was orgasm or not. Different people can have different heart rate responses to orgasm. For example, consider the variability observed by other researchers investigating heart rate during self-reported orgasms in the tables below.
- Bohlen (1984) shows heart rate variability of 102 ±16 beats per minute for orgasm with self-stimulation and with large increases in heart rate based on positions like the woman-on-top and man-on-top coitus.
- Alzate, Useche, and Villegas (1989), using heart rate as an indicator of orgasm, reported values barely above 100 bpm, falling short of Hartman and Fithian’s approximately 120 bpm threshold.
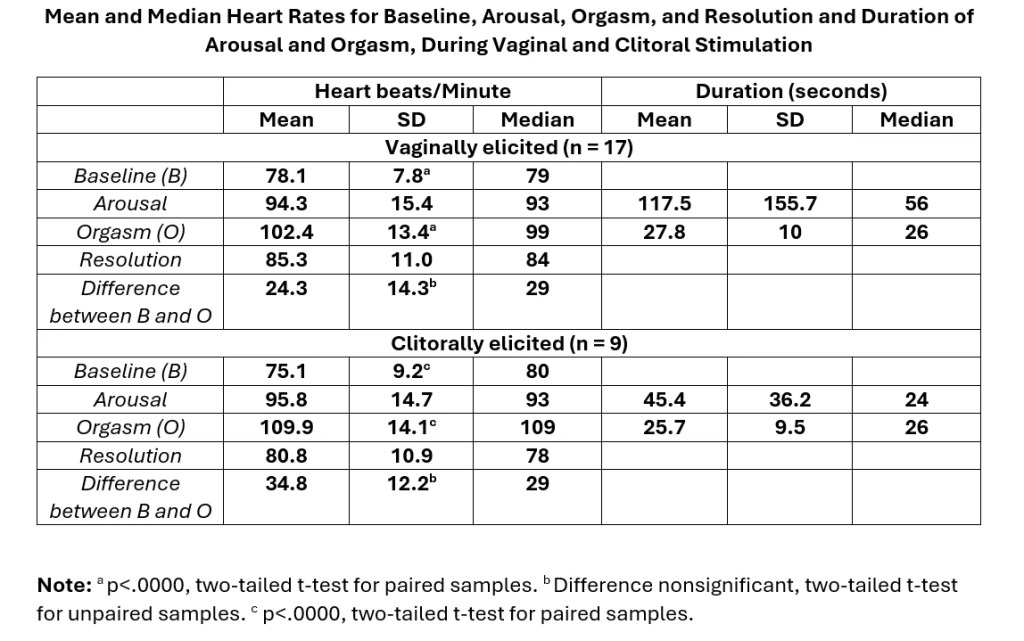
Unlike Hartman and Fithian’s study, both studies used subjective reports as an indicator along with heartbeat. However, subjective report is also problematic since some women tend to think they are orgasming but are not having an orgasm as found by Nicole Prause (in press; see Covert, 2017; Weiss, 2018).
The rhythmic urogenital reflex is currently the gold standard for orgasm detection, which has view confounding factors (e.g., it can occur to some extent high plateau phase in advanced edgers; may be weak in some individuals). Although Hartman and Fithian (1984) note that “pelvic contractions coincided with the elevation of heart rate at orgasm” (p. 159), they never represent any of these pelvic floor contractions. This is likely due to lack of good probe technology in the 1970s. Pelvic floor contractions can also mean pelvic floor tension and relaxation rather than the urogenital reflex, so it is unclear if Hartman and Fithian looked for just any contraction or the stereotyped urogenital reflex. The “patterns” likely reflect variations in autonomic response rather than different “types” of orgasms. The “fingerprinting effect” they noted reflects individual variation in secondary characteristics rather than “types” of the primary event. They are correct in their male/female similarity observations, which support the common neural circuit basis. This reinforces why we need to focus on the actual neural circuit patterns (probe, FMRI, EEG, future technologies) rather than variable physiological markers that can be influenced by many factors beyond the core phenomenon.
Hartman and Fithian’s “Multiple Orgasm” Typology
If heart rate cannot reliably detect orgasm, how is it supposed to detect multiple orgasms? The misguided conclusion from their publication in The Physiologist appears to have convinced them to rely exclusively on heart rate measurements from thereon. Certainly, it is much easier to hook people up to one monitor rather than multiple monitors, so this could have been preferred. This conclusion ultimately resulted in their creation of the “multiorgasm continuous” and “multiorgasm discrete” classifications for both males and females in their 1984 publication Any Man Can. This shift away from comprehensive physiological monitoring to a single, less reliable metric undermined the scientific validity of their later findings.
Hartman and Fithian describe the autonomic patterns as follows:
“We use heart-rate peak as the clearest method of identifying orgasm. Usually the heart rate at rest will be about 70 beats per minute. It will speed up to about 120 beats during orgasm, and return to 70 beats when orgasm is over. A typical chart of a female during orgasm resembles a bell-shaped curve, with the actual duration of orgasm usually being from about six to thirty seconds. The longest orgasm observed lasted one minute. Some women have several such peaks, interspersed with “valleys.” We call such repeating of orgasms multiple orgasms, discrete (see page 160). That is, they start at “rest,” or baseline, reach a peak, and return to baseline before an-other peak occurs. -: Another group of women have an entirely different pattern of multiple orgasms. Their heart rates do not drop to baseline between peaks, but stay high. This is called multi-orgasms, continuous. Yet the peaks are easily identified both by us and by the subjects (see page-161). Another pattern we find is one where the woman has a number of discrete orgasms and then a multi-orgasm with little drop in heartbeat between peaks. Probably because of the emphasis placed on female response during the years of our research, we have far more samples from female subjects than from males. However, even with our smaller male samplings we can detect certain definite similarities between male and female responses. Though individual reactions indicate a “fingerprinting” effect of sexual response for any one individual, there are still certain overall patterns that can easily be identified. It has become clear to us that the similarities between male and female sexual responses are far greater than most people expect them to be.” (Hartman & Fithian, 1984, p. 4-5).
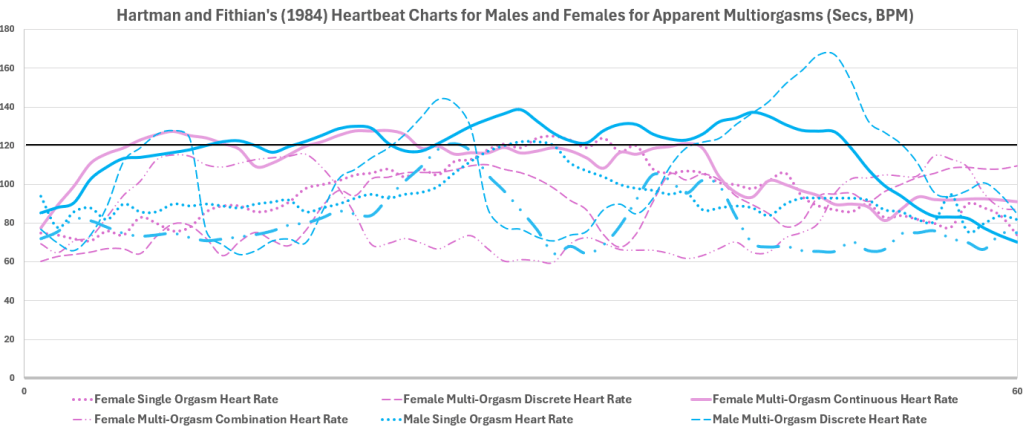
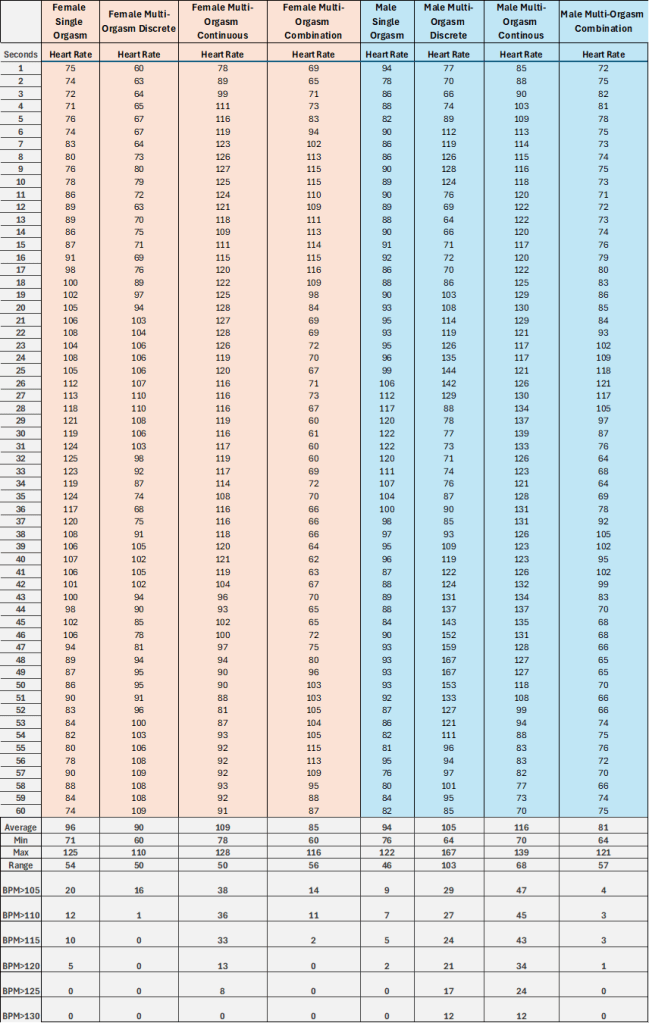
In the research section of Any Man Can, Hartman and Fithian (1984) provided graphs of the apparent multiorgasm patterns. Because this was not a formal academic publication, details regarding participant age, stimulation methods, and experimental procedures—typically included in scientific papers—were omitted. It is unknown whether the data was from the same person or multiple people. I recreated their graphs in higher definition and produced a data set using Web Plot Digitizer at Automeris.io.
The graphs show males and females that had 3 apparent “continuous multiple orgasms” in 1 minute as well as single, discrete, and a mix of the two heart rate patterns.
The Female “Record” of 134 Heartbeat Peaks
In Life as a Sexologist by William Hartman in Bullough et al. (1997), Hartman admits to not validating the 134 orgasm case with a rectal probe and also notes the Berry Campbell’s skepticism:
“We recorded 134 orgasms during a fifty-minute research session with a female volunteer. Upon studying the chart our physiologist [Berry Campbell] was unconvinced that so many separate orgasms had been recorded. He reevaluated the chart and changed his mind after three other subjects had a similar pattern. Did she have 134 separate orgasms with 134 contractions? This is our current thinking, but future research might well define and monitor status orgasmus as well. This refers to subjects entering and remaining in a state of orgasm for extended periods of time. Pelvic contractions of subjects are not easily monitored since some start contractions easily and stop after orgasm. Others begin when the orgasm reaches a high degree of intensity but continue on long after the cardiac data indicate that orgasm is technically over. Some subjects tighten their muscles to bring on the orgasm so contractions occur on a tightened muscle. In all these situations a sharp, clear pattern of contractions is not present” (p. 211).
Berry Campbell’s conclusion that other people had the same orgasm pattern and therefore this participant likely had 134 orgasms, ignores the fact that heartrate is a poor indicator of orgasm. Hartman’s remark about the difficulty of monitoring pelvic floor contractions could have been owed to the state of technology at the time. With today’s sensor technology, researchers like Nicole Prause, who use probe data can distinguish between faked contractions, tensing up, and the urogenital reflex. I have also attempted to fake contractions, tense hard during orgasm, dance around, and manipulate Nicole Prause’s probe without success. The urogenital reflex is distinguishable. This contrasts with Bohlen et al.’s (1980, 1982a, 1982b) work, which clearly documented the contractions. There would also be far more than 134 contractions, it would be more like 10+ contractions per evocation, so a total of 1340+ contractions. It appears Hartman and Fithian know what an orgasm is based on their definition in the earlier section, but they didn’t find what they were looking for due to their uncontrolled methodology. If the participant also claimed that number of orgasms, it is possible that she was reporting peaking sensations or instances of tension/release rather than the occurrence of a specific neurophysiological event.
Hartman’s comments about the mismatch in reported orgasm or another indicator is not much of an error. Rather have a few second margin of error using contraction data than misidentifying orgasm entirely using heartrate. Given that Hartman asked the question about the 134 contractions, it can be inferred that they only used heart rate for this participant. Seeing patterns in other subjects is not good evidence, as Nicole Prause (in press) found her female participants who report multiple orgasms did not have the stereotyped urogenital reflex occur with orgasm (and, more rarely, in high plateau phase in male and females).
Orgasm is not a state nor a feeling but a distinct point marked necessarily that transfers from high neural excitation in specific spinal and brain regions to neural inhibition in both males and females. Kevin McKenna and Lesley Marson‘s work in male and female rats using transneuronal tracing techniques to map pathways of the urogenital reflex would allow these to be mapped in humans, but the ethics of viral mapping techniques deter its use in humans. What they are calling orgasm here seems to be perception of high plateau phase sensory and autonomic dynamics.
Many people think orgasm is a sensation based on qualia or “lived experience,” so they might report sensational peaks that correspond to high heart rate as orgasms. I suspect that the 134 reports of orgasm can be owed to a case of a female who exhibited some autonomic dynamics, but unconvincing evidence of 134 orgasms. Hartman and Fithian seemingly abandoned their self-report button, so it appears that the individual might have been surprised when they were told the results of the 134 orgasms. It is possible that this participant, like Prause’s participants that reported double-digit orgasms (Covert, 2017; Weiss, 2018), didn’t have a single climax just thought they did, or in the Hartman-Fithan case, just had a heartbeat around 120 BPM.
The Male Record of 16 Heartbeat Peaks
Hartman and Fithian (1984) write the following about their male multiorgasm considerations:
“While researching, our next thought was this: Since women are singularly and continuously multi-orgasmic and male and female genitalia develop from the same embryonic tissue, was it not possible that men could also be multi-orgasmic? Physiologists and other experts we consulted with said no because a man ejaculates when he has orgasm —a finite amount of ejaculate puts a limit on number of orgasms. Mrs. Fithian felt that did not settle the matter since male and female function were so much alike and came from the same embryonic tissue; it seemed unlikely they would be so different in regard to multiple orgasms. Several things then happened at approximately the same time. About 1970 a newspaper article said that males taking the drug Mellaril had retarded ejaculation. We encountered two atypical clients in therapy; one had ejaculation without having orgasm, and the other had the sensation of orgasm but didn’t ejaculate. It became obvious that ejaculation and orgasm were not the same thing, and that you could then have one without the other. It stood to reason that males could be multi-orgasmic just as females were. The subsequent ten years of research and working with more clients with these problems have shown this to be true. We have also found, in reviewing early literature, various references to Kinsey’s work and his findings on the separation of orgasm from ejaculation. In comparing male function to that of the female the following records can be compared with the previous female patterns. The more typical male pattern of orgasm is the single orgasm, just as it is in females. In those males who are multi-orgasmic, various patterns emerge just as they did in the female. The following male record shows a series of discrete male orgasms. With this particular subject, ejaculation did not occur at each orgasm, although ejaculation may occur with each orgasm or some orgasms and not others, depending upon the research subject. As you can see, the multi-orgasmic male patterns are similar to that of the female. We know much more about female responses since we have so many more records of female orgasms to study, and multi-orgasmic male responses are fewer in number. We do have a sufficient quantity of records to realize that multi-orgasms are more common than has generally been considered. The fact that multiple orgasms are learned also makes them teachable” (Hartman & Fithian, 1984, p. 163-165)
Heartbeat alone was used for the males as well, so the 16 orgasm in an hour record is also likely an artifact. The lower number could be due less effort being needed to orgasm for the male participant, or simply the male participant having a lower heart rate. It is unclear, as few details are included. Because this sample of males could have included those who have mastered techniques popularized by Robbin and Jensen (1978) like start-stop edging and kegels, it is also important that males be assessed by rectal probe to see if the threshold for the urogenital reflex is met at each time. The urogenital reflex would indicate either orgasm or, more rarely, non-refractory high-plateau phase evocations of this urogenital reflex as seen in Robbin and Jensen (1978). Although one might be tempted to trust the male data as it is usually paired with ejaculation, a highly probabilistic correlate of orgasm (except in cases of non-refractory ejaculatory responses), the fact that they were looking for males who can have non-ejaculatory responses, the male data cannot be trusted as evidence of orgasm.
Continuous Orgasms are not Possible, but Discrete are.
“Continuous multiple orgasms” are not even possible given that orgasm is neurophysiologically discrete event. Even if there were orgasms seconds apart, these would be two discrete events with any “continuous” perception being an illusion. All reflexes have some refractory period, making them discrete. Sensations can be perceived continuously, however. Perhaps there can be some discrete evocations close together one after the other. My recent binary contraction analysis of multiple urogenital reflex evocations, a gold standard correlate for orgasm (most cases)/extremely high plateau phase response (rarer), did not show anything that looked continuous with a 39 second break. It appears the whole “continuous orgasm” idea describes the consciousness of sensory dynamics as well as the ability to maintain heartbeat above or around 120 beats per minute rather than some “type of orgasm” or variation in the orgasm itself. It is possible the individuals had bout of intense stimulation followed by relaxation repeatedly, which can account for the “discreteness.” The “continuousness” can be attributed to sustained intensity of stimulation, especially with use of a sex toy, something the female participants were more likely to use. No notes even describe what the individuals were doing for the given orgasm.
Expected Data for Extreme Orgasm Claims
If the cases of 134 female and 16 male orgasms in an hour were legitimate, what would the data look like? Since 134 is the most highest number, I will use this to emphasize the bizarre factor.
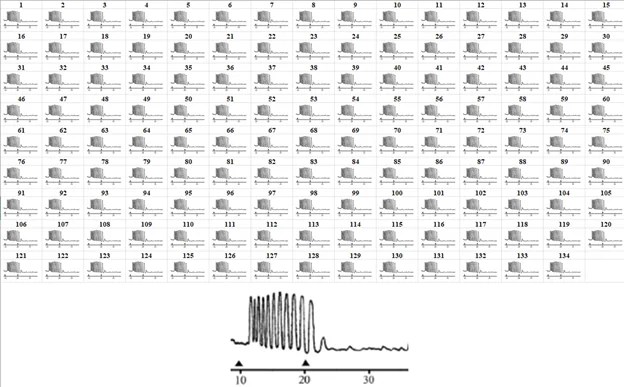
Recreating Heartbeat Data
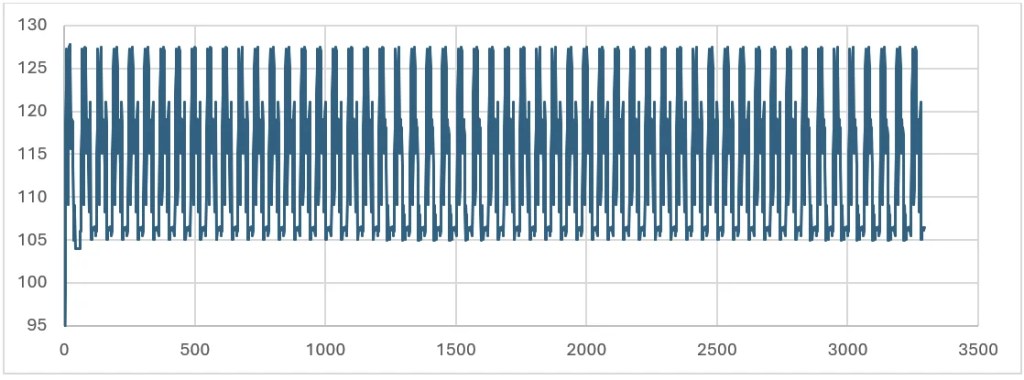
Let’s start with what Hartman and Fithian might have seen on their Beckman dynograph receipt paper. To recreate the printout, I have took the minute data and assumed that there might be some continuous and some discreet in the mix. I scaled the female continuous orgasms examples to equal 134 orgasms in an hour. Although these could be from entirely different people, it could be a good approximation of the printout that Hartman and Fithian (1984) saw. If each minute of print was 10 inches, then the data scroll could be as long as 50 feet, which would be a lot to represent. If 134 one-minute graphs were represented, assuming the size of the images in the Appendix, then 45 pages would be dedicated to this data. Certainly, they wouldn’t want to photocopy a mile-long receipt of data for publication, but it would have been certainly nice to see. Below is the Hartman and Fithian recreated receipt showing 134 peaks in heartbeat.
134 Peak Heartbeat Instances with a Mix of Discrete and Combined Examples (Seconds, BPM)
Recreating Record Based on Rhythmic Urogenital Reflex
Gold standard evidence would involve 134 evocations of the urogenital reflex, which can be measured by an anal probe. In the figure below, I replicated a 10-second evocation of the urogenital reflex 134 times to equal 134 instances.
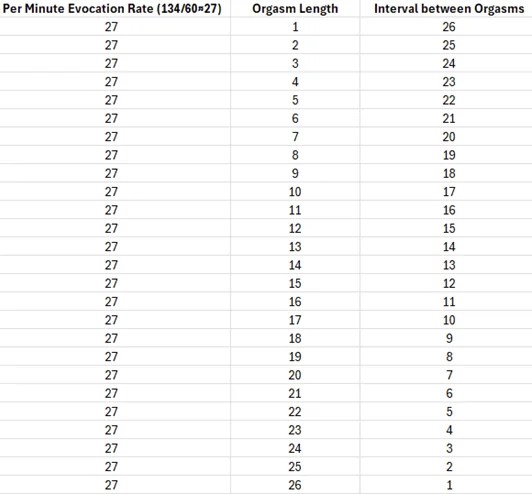
Relationship between Orgasm Length and Orgasm Interval
Having 134 orgasms in 50 minutes to an hour means that orgasms need to be short to fit in the time span. It’s advantageous to minimize the length of orgasms and short intervals for such a record. The longer the orgasm, the less time in between orgasms there is. The shorter the orgasm, the more time in between orgasms there is.
Relationship between Orgasm Length and Orgasm Interval
Data in light of MultipleOs (2024) Binary Contraction Analysis Results
Binary contraction analysis is a rule-of-thumb approach that involves marking each contraction in single-shot, slowed-down porn videos of the anus during claimed orgasm with a 1 and all other values with a zero with corresponding time in milliseconds to graph and analyze the length, interval distribution, and other metrics of the urogenital reflex during claimed orgasm. For instance, visible contractions on Reddit’s r/orgasmiccontractions and r/gayorgasmcontractions are exemplary.
The results of the first binary contraction analysis (MultipleOs, 2024) are in stark contrast with reported figure of 134 orgasms claimed in the Hartman-Fithian research. In an analysis of publicly available adult content, documented examples of urogenital contractions indicating orgasm have not exceeded six to seven occurrences per individual session (MultipleOs, 2024). In the binary contraction analysis, neither female had 27 second intervals, and these are stand-out record cases. In addition, Female 2, who had the shortest interval between evocations of the urogenital reflex, a gold-standard correlate of orgasm, had intervals that consistently increased overtime from 39.25 seconds to 99.5 seconds. Because the urogenital reflex can also occur in high plateau phase in is possible some of these instances are not orgasm but high plateau phase evocations. The large disparity between these documented cases and Hartman and Fithian’s findings further calls into question the validity of their measurements and conclusions.
For reference, a binary contraction analysis with 134 would look like the following, assuming a 10-second orgasm:
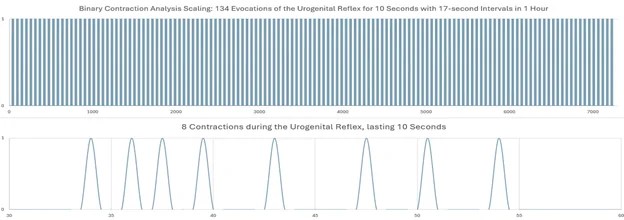
The figure of 134 orgasms represents approximately a twenty-fold increase from the documented maximum of 6-7 orgasms (MultipleOs), or specifically, it is 19-22 times higher than those with the stronger correlate of the urogenital reflex. This dramatic difference—an increase of roughly 2000%—highlights the likely implausibility of the Hartman-Fithian findings when compared to observable physiological evidence. Such a substantial disparity suggests their methodology likely captured other physiological responses rather than actual orgasmic events.
The binary contraction analysis so far shows the most available evidence of orgasm in not only literature but pornographic content, with the opposite. Many male videos with ejaculation as another good correlate were not included due to not showing the anus. For instance, Reddit’s r/ruinedorgasmsplus shows some males having back-to-back-to-back non-refractory ejaculations in a single shot, unedited video which usually occur with the urogenital reflex in less than a minute. There are also a few instances of female videos where 2 orgasms are had in a minute, but there is no evidence of this being sustained for an hour in 1000s of videos labeled “multiple orgasms.” There are also several videos where no anus is shown for females that claim double-digit or triple-digit orgasms, but so far, the verdict is still out for whether they are actually having many orgasms or even a single orgasm. All in all, the true record numbers backed by gold-standard contraction data are likely far closer to the binary contraction analysis study. More research is needed to determine what the true potential is for various time ranges including 10 minutes, 30 minutes, an hour, and multiple hours.
Other Claims of Hundreds of Orgasms
A recently published survey study reported the maximum number of orgasms participants experienced in a single sexual activity session ranged from 3 to 10, as reported by five participants. The other seven participants described that they experienced uncountable orgasms in a single sexual activity session, such as “unlimited”, “100+”, “beyond count”, or “can last over two hours” (Corre, Rapsey, & Wibowo, 2025). In Reddit communities like r/multiorgasmic, several male and female individuals claim 100s of orgasms. People tend to create their own definition of orgasm without care about whether it corresponds to neurophysiology or not. A member of this community and a participant of the study, I have incorrectly claimed 100 orgasms as well, counting sensations felt like orgasm perceived over and over again as orgasms. I used feeling-based definitions often used by researchers like Umit Sayin (2019) and Whipple and Komisaruk (2011). I was also using Robbin and Jensen’s (1978) “non-ejaculatory orgasm” definition, involving evocation of the urogenital reflex (also called orgasmic contractions) without transitioning into refractory inhibition. I considered these different “types of orgasms.” Thus, I am guilty of using the common qualia-based definition in the past where peaks of sensation or tension-release instances are called orgasms and thought of “types of orgasms” based on where they are felt. This is likely what others are also doing.
While there are numerous accounts of individuals who report hundreds of orgasms per session or per hour (e.g., Sayin, 2019; Shtarkshall, Anonymous, & Feldman. 2008), the accounts in these studies only use subjective report. Furthermore, several media reports of individuals with persistent sexual arousal disorder (PSAD)/restless genital syndrome also report hundreds of orgasms per day. However, no clinical validation with rectal probe has even been done involving these individuals. It is crucial to note that the term “orgasm” is frequently misapplied to describe intense sensory processing rather than being reserved for the specific neurophysiological event characterized by activation of the Onuf’s nucleus and the resulting urogenital reflex and transition from high neuronal excitation to inhibition. This distinction is particularly important when considering PGAD, which, contrary to sensationalized media reports, is primarily characterized by persistent pelvic discomfort or pain. Contrary to popular belief, PGAD neither guarantees multiple orgasms nor necessarily includes orgasmic capability at all—in fact, some individuals with this condition may experience an inability to achieve orgasm (anorgasmia).
Conclusion
While I appreciate Campbell, Hartman, and Fithian for their pioneering contributions to sex therapy, as a scientist, I cannot help but to maintain a skepticism of the apparent blunder in their research: use of heartbeat alone for evidence of orgasm in determining the 134-orgasm record. While there is a growing trend in “lived experience” research and changing conclusions as to not invalidate someone’s experience, if the experience is not supported by gold-standard evidence, we as scientists need to be willing to say that whatever was experienced is not an orgasm. Bohlen et al. (1982) had a female participant who reported orgasm but there were no contractions, which the authors called a “type of orgasm,” erroneously, or perhaps not to make people feel invalidated. Unlike Nicole Prause, who cares more about determining what is occurring rather than people’s intuitions about what has occurred, Bohlen et al. (1982) might not have had the guts to say they were not orgasms, which would have a lot of implications for a harder stance and would potentially classify many females previously classified as “functional” as “dysfunctional.” While people often think they can define “what orgasm is for them,” as sometime recommended by sex therapists/sexperts, this is simply language and conceptual games with no grounding in the neurophysiology. What makes someone feel better doesn’t mean it’s true. It is not to say their experience is not profound, pleasurable, or something else, but it is certainly, by the preponderance of evidence, not an orgasm.
Hartman and Fithian (1984) performed most of their studies in the 1970s, likely before any reliable research probe, such as one of Bohlen et al. (1978) was made. The researchers used what they had at the time technology-wise, and it is not the state of their technology I am criticizing nor their attempts to use such technology, but their later sole reliance on heartbeat and, even more so, our contemporary trust placed in their findings like their unvalidated claim of 134 orgasms in an hour, which appears highly likely to be an artifact rather than a finding of their studies. Hartman and Fithian were correct about many areas of physiology, including the similarity in female and male response. Researchers should stop citing their apparent record in their work. If anything, they should be cited as an example of why heartbeat alone is a poor indicator that orgasm occurred similar to how statistic professors use Kinsey interview methods as a teaching lesson for how not to do a sample.
References
Alzate, H., Useche, B., & Villegas, M. (1989). Heart rate change as evidence for vaginally elicited orgasm and orgasm intensity. Annals of sex research, 2(4), 345-357.
Bohlen, J. G., & Held, J. P. (1979). An anal probe for monitoring vascular and muscular events during sexual response. Psychophysiology, 16(3), 318-323.
Bohlen, J. G., Held, J. P., & Sanderson, M. O. (1980). The male orgasm: pelvic contractions measured by anal probe. Archives of Sexual Behavior, 9(6), 503-521.
Bohlen, J. G., Held, J. P., Sanderson, M. O., & Ahlgren, A. (1982a). The female orgasm: Pelvic contractions. Archives of Sexual Behavior, 11, 367-386.
Bohlen, J. G., Held, J. P., Sanderson, M. O., & Boyer, C. M. (1982b). Development of a woman’s multiple orgasm pattern: A research case report.
Bullough, V. L. & Bullough, B. (1994; 2013). Human Sexuality: An Encyclopedia. Retrieved from https://files.acearchive.lgbt/artifacts/bullough-human-sexuality/human-sexuality-an-encyclopedia.pdf
Campbell, B., Hartman, W. E., Fithian, M., & Campbell, I. (1975). Polygraphic survey of the human sexual response. The Physiologist, 18(3), 154.
Chalker, R. (1994). Updating the model of female sexuality. SIECUS Report, 22(5), 1-6.
Corre, P. H. C., Rapsey, C. M., & Wibowo, E. (2025). Description of how men achieve multiple orgasms. Sexual and Relationship Therapy, 1–13. https://doi.org/10.1080/14681994.2025.2451995
Covert, J. (2017). Inside the Orgasm Lab. Retrieved from https://www.menshealth.com/sex-women/a18770869/female-orgasm-study-research/
Hartman, W. E., & Fithian, M. (1979). The Development of A Treatment Program for Sexual Dysfunction at the Centre for Marital and Sexual Studies’. The Frontiers of Sex Research, 13.
Hartman, W.E. and Fithian, M.A. (n.d.). Rationale on Multiorgasm. In Kothari and Patel, op. cit., 215.
Komisaruk, B. R., & Whipple, B. (2011). Non-genital orgasms. Sexual and Relationship Therapy, 26(4), 356–372. https://doi.org/10.1080/14681994.2011.649252
Robbins, M. B., & Jensen, G. D. (1978). Multiple orgasm in males. Journal of Sex Research, 14(1), 21-26.
Sayin, H. U. (2019). Five Cases with Expanded Sexual Response (ESR). Ann Clin Case Stud, 1(1), 1005.
Shtarkshall, R. A., Anonymous, & Feldman, B. S. (2008). A woman with a high capacity for multi-orgasms: a non-clinical case-report study. Sexual and Relationship Therapy, 23(3), 259-269.
Weiss, S. (2018). Some People’s Orgasms Are Actually a Series of Short Ones. Vice. Retrieved from https://www.vice.com/en/article/7xqq4g/women-short-orgasms
World Sex Records. (1997). Sexual Records. Retrieved from https://web.archive.org/web/19991127171514/http://www.sexualrecords.com/WSRtechnique.html

Leave a comment