Introduction
Sixty years ago, Masters and Johnson recorded videos of pelvic floor contractions for their 1966 study. The Kinsey Institute has an example of these videos, filmed with old film technology. Unfortunately, Masters destroyed most of his data, so it cannot be peer-reviewed and further understood. Fortunately, today, we have the luxury of millions of high-definition, pornographic content with close-ups of the contractions, making binary contraction analysis possible (e.g., r/orgasmiccontractions).
Methods
In this binary contraction analysis study, I review multiple evocations of the urogenital reflex, a gold-standard correlate and an expected part of neurophysiological orgasm in individuals without spinal cord injury. I reviewed thousands of videos and included those with the highest number of visually verifiable evocations in males and females. Search terms included “multiple orgasms,” “orgasmic contractions,” “male multiple orgasms,” “back-to-back orgasms,” “forced orgasms,” “real female orgasms,” and “ruined orgasms.” Sites reviewed included FTV Girls, The Female Orgasm, Hegre Art, Kink.com, and amateur content on OnlyFans and Pornhub, xHamster, xVideos, and other platforms. All videos that met the criteria were amateur videos rather than those produced by productions. However, there are a few notable instances on each site observed of 2 or 3 evocations.
Two females with 6 evocations and one male with 7 evocations video met the selection criteria: acceptable lighting, multiple instances of visible contractions within at least five minutes of each other, and a single-shot video without cuts or changes in camera angle. Videos showing repeated evocations were considerably rare. In fact, many reporting very high numbers of orgasms were not exhibiting a single instance of contractions, a finding recently reported by Nicole Prause (in press) using a rectal pneumatic micropressure sensor probe. Although there are thousands of videos of male back-to-back ruined orgasm, almost all of them focus on the penis rather than the anus. In contrast, many videos of females focus on the vaginal which will also clearly show the anus.
The videos were slowed down to .25 times for more accurate time-stamping in Excel. Peak contractions were each marked with a 1 and all other time instances are marked with a 0, which create decent. The estimated margin of error is + or -.25 seconds for time marks. The margin of error for the number of contractions is estimated to be + or – 3, which will also affect orgasm length. Use of the bulbocavernosus muscle was used for a few contractions for instances where the butt was clenched or in poor lighting, hiding visibility of the anus. The genital sensation perception that usually occurs with orgasm (except in anhedonic orgasm, some spinal cord injuries) usually starts a few seconds before the first contractions and subsides in the last few contractions. The margin of error in terms of sensation perception is estimated to be + or – 5 seconds.
Data
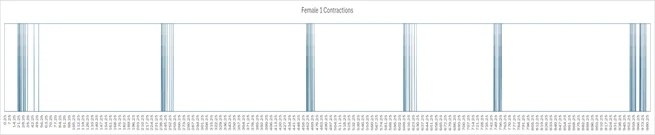
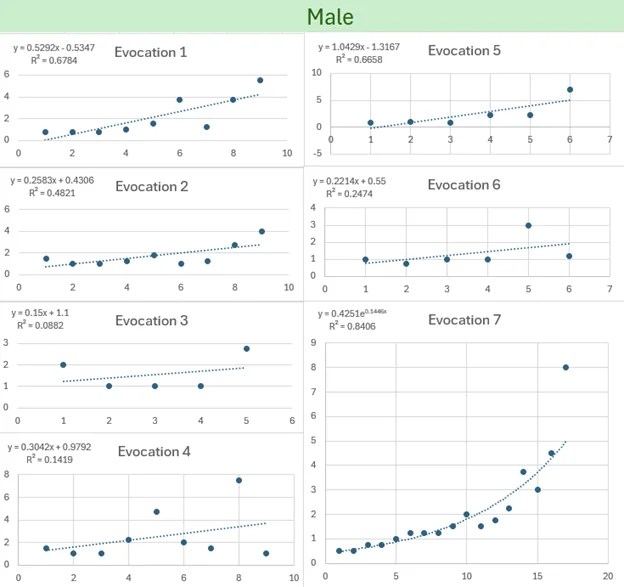
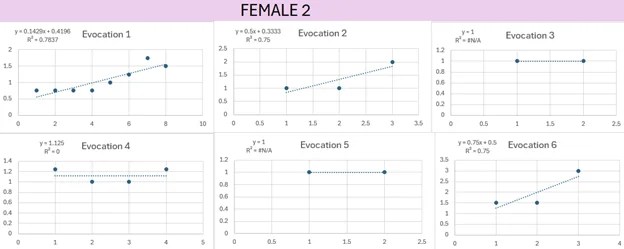
The following graphs show the results of the binary contraction analysis. The video and raw data can be viewed here.




Linking in Prior Studies
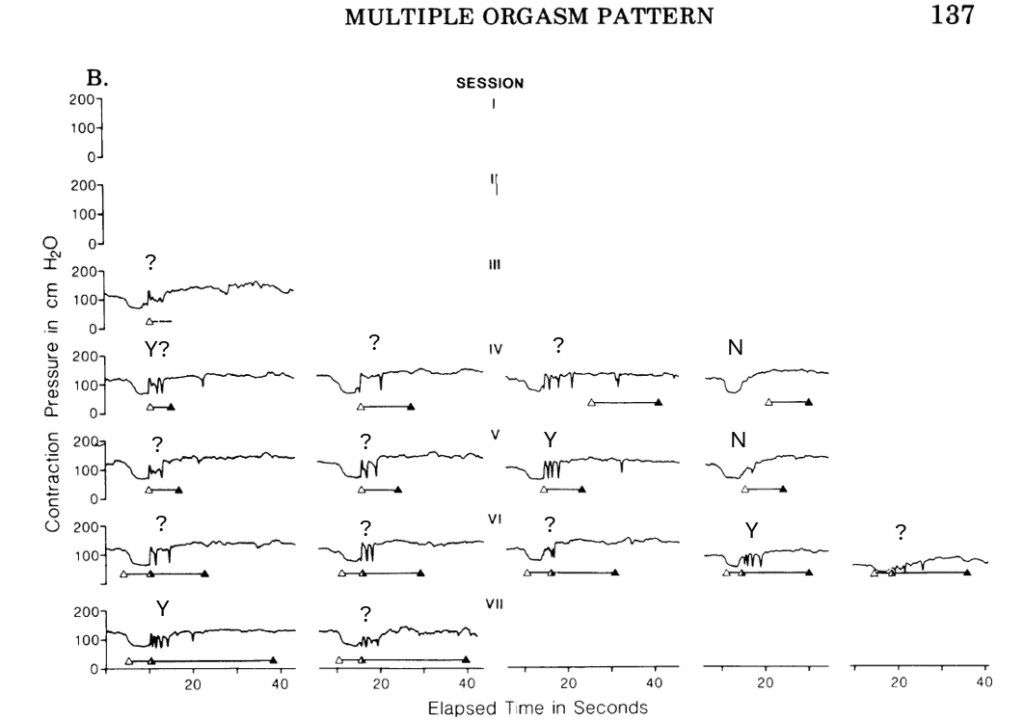
Two prior studies showed contraction data for three or more orgasms. Bohlen et al. (1982) featured a single woman that attempted to have multiple orgasms, which were measured by a rectal probe. Robbins and Jensen (1978) published rectal contraction data from one male participant who reported multiple orgasms with contractions.
Bohlen et al. (1982) used an inflatable probe, so the contractions show decreases in pressure rather than increases, which is why the period after orgasm has higher pressure than the regions during orgasm. Like Female 2 in the study, some reported orgasms only had a few contractions, yet a few are more stereotyped like Session VII, evocation 1.
To assess whether the data aligns with the urogenital reflex, I’ve added labels:
- Y: Indicates a pattern consistent with the urogenital reflex (hard, rapid contractions with decreasing pressure over time).
- N: Indicates a pattern inconsistent with the urogenital reflex.
- ?: Indicates an inconclusive pattern.
Based on these criteria, it seems that Bohlen et al.’s (1982) data might be difficult to interpret due to either:
- Probe limitations: The inflatable probe may have hindered accurate pressure measurement.
- Short or irregular contractions: The female participants’ contractions could have been too brief or inconsistent for clear analysis.
In contrast, modern techniques using silicone tubing and micropressure sensors often provide more distinct and interpretable patterns. Similarly, Robbin and Jensen’s (1978) published data on a male participant also presents challenges in identifying clear urogenital reflex patterns. Below are images from Bohlen et al. (1982) and Robben and Jensen’s (1978) studies, respectively.


Example of Modern High-Quality Output with the Urogenital Reflex, using Prause and Arnold’s Rectal Probe and Arduino Setup
Analysis
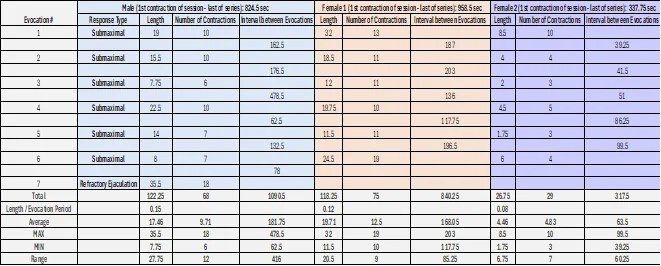
The male exhibited the highest number of evocations (7). Following six non-refractory evocations of the urogenital reflex, the male experienced a refractory ejaculation characterized by:
- Rapid loss of erection
- Notably intense and prolonged contractions compared to previous submaximal threshold evocations
- Increased relaxation
The male also displayed the greatest variation in both contraction length (7.75 to 35.5 seconds) and number of contractions (6 to 18). The refractory ejaculatory orgasm involved a higher number of contractions, which were visibly more powerful than the preceding submaximal threshold responses.
I hypothesize that all females experienced maximal threshold responses, as evidenced by post-evocation clitoral hypersensitivity. This likely led to a refractory period due to neuronal inhibition, unlike the submaximal threshold responses observed in males without neural inhibition.
However, given the threshold discordance of spinal cord reflexes and the upper bound threshold of neural inhibition, it is possible that Female 2 exhibited a few submaximal threshold evocations of the urogenital reflex through edging. Urogenital technique through edging might correspond to fewer contractions.
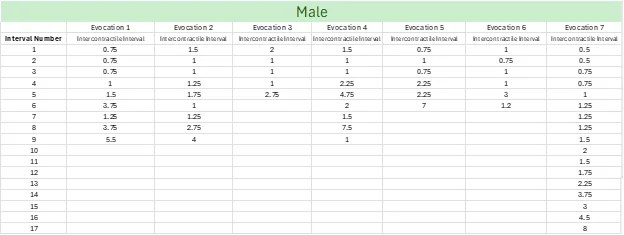
Female 1 exhibited the highest average number of contractions per session (12.1), followed by Male (9.71) and Female 2 (4.83). Evocation 6 of Female 1 demonstrated two regular, rhythmic contractions with a five-second break in between, suggesting a pattern consistent with the Type III category described by Bohlen et al. (1982). Female 1 also had the longest average contraction duration (17.46 seconds), followed by Male (19.71 seconds) and Female 2 (4.83 seconds). In terms of total contraction duration, the male led with 122.25 seconds, followed by Female 1 (118.25 seconds) and Female 2 (26.75 seconds). The male’s refractory ejaculatory orgasm featured the most contractions and the longest duration.
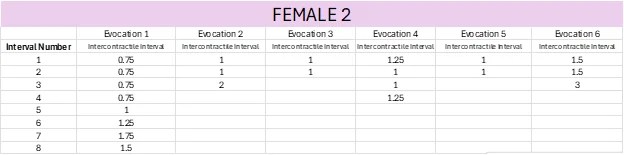
Female 2 had the shortest evocation period (first contraction to last of series) and the shortest time between evocations (e.g., 39.25 seconds). Interestingly, the time between orgasms increased with each successive one, a trend not observed in Female 1. Even if Female 2 could maintain this rate of evocation, considering the potential for increased neural inhibition with each session, her total evocation length might still not surpass that of Male or Female 1.
Several of Female 2’s evocations were questionable in terms of whether they represented the urogenital reflex as were some of the contractions in Bohlen et al. (1982) study. Some instances lasted only 1.75 seconds and involved just three contractions, possibly indicative of the anal wink reflex or vaginal throbbing dynamics. It is conceivable that a few of these contractions were not visually apparent but might be detectable using an anal probe, a gold-standard research tool.
These instances raise the question of whether there should be a minimum number of contractions to qualify as a urogenital reflex. Literature often cites a range of 3 to 15 contractions (e.g., Kratochvil, 1994; Masters and Johnson, 1966). A cutoff of 3 contractions seems reasonable, but it is relatively easier to stimulate compared to the 18 contractions observed in the male’s Evocation 7 or the 19 in Female 2’s Evocation 6. If a 6-contraction cutoff were applied, five of Female 2’s evocations would not be classified as urogenital reflexes.
Limitations
Limitations of this study include the previously mentioned margins of error. Visibility issues such as shadows, anal color, camera angle, lighting, movement, anal cheek closure, anal hole shape, anal winking, and potential voluntary contractions toward the end of involuntary rhythmic contractions can affect data accuracy.
None of the excluded female videos exhibited a higher number of actual evocations than those selected. A few male videos only captured a frontal view of multiple non-refractory evocations (up to 10 times), each followed by ejaculation within 5 minutes. Additionally, some males displayed a short refractory period with 2 to 3 maximal threshold responses within 5 minutes, each followed by rapid state deviation and complete loss of erection.
Male videos tended to focus on the penis rather than the anus, resulting in a smaller sample size compared to female videos, which often focused on the vagina. The lighting in most female videos was also significantly better, further limiting the availability of male videos for binary contraction analysis.
Conclusion
A striking observation when examining the graphical data as a whole is the individuality of each evocation, even within the context of the stereotyped response. While the term “stereotyped” suggests a consistent pattern, the data reveals that each evocation is unique, varying even within the same individual during a single session.
Therefore, typologies like Bohlen et al.’s (1980, 1982) Type I-III serve primarily as a framework for researchers to identify potential patterns rather than as a comprehensive description of the urogenital reflex’s vast variability.
- Type 1: A simple series of regular contractions.
- Male: (6.4 – 31.3 seconds; 8-18 contractions)
- Female: (7.4-15.6 seconds; 8-15 contractions)
- Type 2: Regular series followed by irregular contractions.
- Male: (20.1-56.1 seconds; 13-33 contractions)
- Female: (17.7-107.6 seconds; 9-34 contractions)
- Type 3: Preliminary contractions preceding a series of regular contractions mid-orgasm.
- Male: (25 seconds; no dispersion indices)
- Female: (unknown, unknown)
- Type 4: No contractions despite reported orgasm.
- Male: (unknown, N/A)
- Female: (24.4, N/A)
Note that Type 4 should not be considered a type of urogenital reflex or evidence of orgasm, except perhaps in cases of spinal cord injury with sacral region damage. While previously observed only in females, recent trends have seen males adopting expanded definitions of orgasm to encompass highly pleasurable experiences and sensations, including non-orgasmic or merely orgasmic correlates without orgasm.
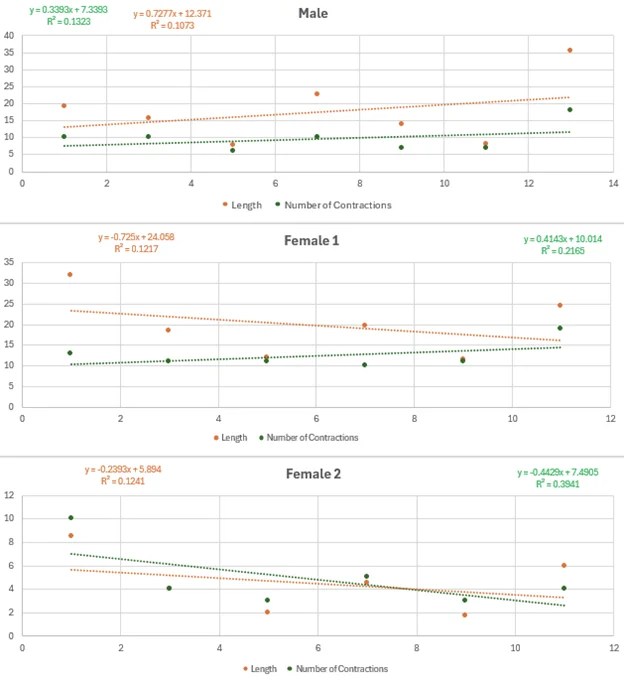
I’m currently developing a novel neurophysiological model that addresses the emergence of micro-variability within each evocation of the stereotyped macro-level view. Recent consultations with leading experts in the human and animal urogenital reflex revealed that it is unknown why the urogenital reflex presents the way it does and why there is such variability. While the urogenital reflex is generally stereotyped, particularly in the initial contractions, stochastic dynamics within spinal and network potentiation in neural networks within the sacral spinal cord, bottom-up stimulus processing, and top-down processing could explain such randomness. Overarching generalizations like “orgasms or urogenital correlates tend to become shorter, longer, weaker, stronger, etc., with each evocation” over time are not helpful when modeling the stochastic reality. The low r-squared values observed underscore the randomness of the data and its poor fit to any trendline supporting these generalizations.
In addition to highlighting individual variability, the findings challenge the prevailing assumption of unlimited orgasmic capacity, particularly in women. Contrary to the assertions of authors such as Mary Sherley and Masters & Johnson, our study demonstrates that the human body has physiological limitations regarding the frequency and proximity of orgasms. Female 2 had to wait some time between orgasms and the interorgasmic interval. Seven evocations in the male would also be unexpected by writers like Masters and Johnson (1966) who believed that the males of Robbin’s and Jensen’s study were faking the contractions. Several males in my survey of pornographic content had ruined orgasms 10 seconds or less apart, but they could not be included because of the focus on the penis. Many just showed multiple instances of squirting or a male having a shaking response largely associated with the Aneros community or instances of prostate milking. This suggests that they are having something else they are calling an orgasm, such as any release, any peaking, pleasure, etc. In porn video analysis from sites reporting to only show female multiple orgasms, I found that females report orgasms ten, twenty, or even hundred times, yet show not evocations of the urogenital reflex. While the demand for multi-orgasm content in the adult entertainment industry might suggest otherwise, our analysis did not identify instances of significantly more than seven consecutive orgasms in either sex. Perhaps I missed one. I certainly did not watch all the porn in the world. If so, please DM me.
While binary contraction analysis may not be as precise as a rectal probe, it offers a valuable alternative for studying orgasmic patterns. Compared to anecdotal accounts, binary contraction analysis provides a more objective and quantifiable measure of orgasmic activity. Future research should consider incorporating binary contraction analysis in cases where the use of a rectal probe is impractical or undesirable. This approach could help to elucidate the potential for multiple orgasms and provide a more reliable basis for understanding individual differences in orgasmic experiences. Perhaps there are those out there that can have double or triple orgasms. With binary contraction analysis, individuals now have a easy and cost-effective way to data when they report 100s of orgasms.
References
Bohlen, J. G., Held, J. P., Sanderson, M. O., & Ahlgren, A. (1980). The female orgasm: Pelvic contractions. Archives of Sexual Behavior, 11, 367-386.
Bohlen, J. G., Held, J. P., Sanderson, M. O., & Ahlgren, A. (1982). The female orgasm: Pelvic contractions. Archives of Sexual Behavior, 11, 367-386.
Kratochvíl, S. (1994). Vaginal contractions in female orgasm. Ceskoslovenska Psychiatrie, 90(1), 28-33.
Masters, E. H., & Johnson, V. (1966). Sexual Response. Boston, MA: Little Brown.
Robbins, M. B., & Jensen, G. D. (1978). Multiple orgasm in males. Journal of Sex Research, 14(1), 21-26.
Weiss, S. (2017). No, it’s not “normal” for all people with vaginas to have multiple orgasms. Bustle. Retrieved from https://www.bustle.com/p/not-all-people-with-vaginas-have-multiple-orgasms-this-sex-myth-is-more-problematic-than-you-think-2305091

Leave a comment