Introduction
Male orgasms are typically characterized by rhythmic contractions of the pelvic floor muscles, often accompanied by ejaculation. However, some men report the ability to experience orgasms without ejaculation, commonly called non-ejaculatory orgasms (NEOs) (Wibowo & Wassersug, 2016). The question of whether NEOs and ejaculatory orgasms at the point of no return (PONR) involve the same muscular contractions has been debated in both scientific and non-academic communities. This review compiles available data on male orgasmic contractions to investigate potential differences between submaximal threshold responses (NEOs) and maximal threshold refractory climax contractions with ejaculation. The compiled data reveal inconsistencies in contraction profiles between NEOs and ejaculatory orgasms across individuals. Some studies and anecdotal reports suggest that NEO contractions can be nearly identical to those of ejaculatory orgasms in terms of amplitude, frequency, and duration. Others in online communities (e.g., r/multiorgasmic) indicate activation of the orgasmic reflex during NEOs that results in contractions that differ from those observed during maximal threshold ejaculatory orgasms. I hypothesize that the contractions in the submaximal threshold responses are different in frequency, amplitude, and duration from the maximal threshold refractory response. Given the inconclusiveness of existing data, more research is needed to determine what contractile typologies might exist in this spectrum and how much (if any) spectrum exists.
Background
Definition
A penile non-ejaculatory orgasm (NEO) is a complex multidimensional phenomenon characterized by an orgasmic experience without semen emission. Like the orgasmic response at the PONR, this response integrates sociological, psychological, physiological, and ecosystemic components, resulting in a holistic experience that encompasses individual sensations, personal, religious, and cultural meanings, bodily reflexes, and broader contextual factors. This response integrates psychological and physiological components, resulting in sensations and reflexes typical of orgasm while maintaining ejaculatory control.
In zone theory (See figure below.), a penile non-ejaculatory orgasm is a submaximal threshold response. Submaximal threshold responses, whether or not they involve ejaculation or contractions, do not have a refractory period, making them intriguing for many men seeking to enhance pleasure. Notably, submaximal threshold responses encompass all potential penile reactions below the PONR. Various non-ejaculatory orgasm (NEO) types and non-refractory ejaculatory orgasms are subsets of this broad category of submaximal threshold responses. Similarly, the term “maximal orgasm” might be preferable to “refractory ejaculatory orgasm” to include cases such as retrograde ejaculation, anejaculation, gushing in transgender individuals with neovaginas, and dry orgasms in young males. The characteristics of submaximal threshold types are likely diverse and share multiple dimensions with full ejaculatory orgasms, making clear distinctions between different submaximal threshold types challenging. There is debate about whether a penile NEO must involve pelvic floor contractions (Davidson, 1980). While no specific scale exists for rating non-ejaculatory orgasms, it would likely share many dimensions with Mah and Binik’s (2001) Orgasm Rating Scale:
Sensory aspects—spreading sensations (flowing, spreading, radiating), whole-body involvement (trembling shuddering), ejaculatory sensations (oozing, spurting, shooting), rhythmic sensations (quivering, pulsating, throbbing), release of tension (relieving, releasing, erupting, exploding), buildup of tension (rising, building, swelling), thermal sensations (cool, warm, hot), and miscellaneous (tickling, tingling, flushing), evaluative aspects—feeling of inevitability (inevitable), temporal evaluation (quick, long, unending), intensity (mild, moderate, intense, powerful), physical effects (relaxing, engulfing, exhausting), depth (deep, full, complete), global pleasure (pleasant, enjoyable, pleasurable, incredible), sensual pleasure (soothing, sweet, sensual, exquisite), satisfaction (satisfying, gratifying, fulfilling, cathartic), excitement (exhilarating, exciting, wild), and affective aspects—emotional intimacy (close, loving), joy-peacefulness (peaceful, blissful, tender), joy-elation (elated, ecstatic, euphoric, rapturous, passionate), emotional-excitation (abandon, uncontrolled), emotional fusion (immersing, merging, unifying), unreality (light-headed, dizzy), lack of awareness of surround (detached, oblivious, unreal), suspension (suspended, soaring), and miscellaneous (melting, vulnerable).
Disambiguation with Zone Theory
Many clinicians remain unaware of submaximal threshold responses, as these phenomena fall outside the diagnostics of andrology. Previous research has often conflated non-ejaculatory threshold responses with maximal threshold responses typically associated with sexual dysfunction when antegrade ejaculation is absent (e.g., undifferentiated mentions in Gérard et al., 2021). Previous research has also conflated maximal clitoral response and male submaximal threshold responses like the NEO as homologous responses.
The NEO phenomenon is separate from non-penile sensations sometimes labeled as non-ejaculatory orgasms, such as the set of responses called “Super O” associated with Aneros prostate stimulation, frisson, or anal sensations. NEOs are unique in that they can occur multiple times in succession without triggering a refractory period. It is crucial to differentiate NEOs from other similar-sounding phenomena. Submaximal threshold responses should not be conflated with dry orgasms experienced by prepubescent males or cases of anejaculation during a full climax in adult males. Submaximal threshold male sexual responses, including NEOs, should also be distinguished from multiple female orgasms, which are maximal threshold responses. While these phenomena may share some experiential dimensions, they represent distinct physiological processes. This definition emphasizes the specific nature of penile NEOs as a submaximal threshold orgasmic event, distinguishing them from both full climax experiences and other non-penile sensations often labeled orgasms because of shared dimensions. Understanding this distinction is essential for accurate research and discussion in the field of male sexuality and orgasmic response.
Zone theory can be used to create a language that speaks about the spectrum of male penile responses in a particular way. The below figure represents part of zone theory with a focus on male response.
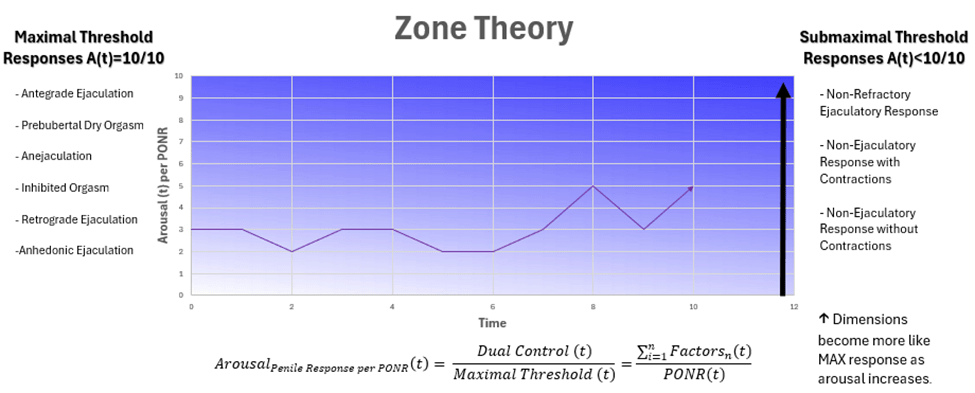
Zone theory models submaximal threshold responses for males and females according to a mathematical dual control model and threshold time series analysis, although only male response is represented here. Janssen and Bancroft (2023) describe the dual control model as follows:
“The dual control model proposes that sexual arousal and related processes are dependent on the balance between sexual excitation and sexual inhibition. In addition, the model proposes that individuals vary in their propensity for these processes…. The idea of regulation by forces and counterforces, or by the interaction between activation and suppression, is not uncommon, for instance, in cognitive and psychophysiological research on memory, general arousal, emotions, and affect. As with the dual control model of sexual response, this generally includes hypotheses about independence or orthogonality. For example, the sympathetic and parasympathetic branches of the autonomic nervous system are traditionally considered to have reciprocal or opposing effects on general arousal processes. Additionally, the notion of “level of analysis” comes to mind when considering control or regulation of sexual response. At a lower, or “molecular,” level, sexual responses are likely controlled by a large number of inhibitory and excitatory neurophysiological processes…. The dual control model represents a higher, or “molar,” level of analysis, which addresses the functions and interaction between sexual arousal and inhibition as a “conceptual nervous system”…. However, the model is primarily a conceptual device, a means of structuring and formulating research questions. Reality is undoubtedly more complex. For instance, even inhibition will require some type of activation. Furthermore, although we assume that inhibitory and excitatory processes, at the trait level, are orthogonal or independent, at the state level, they may not be as disconnected and could potentially modulate each other’s output levels or “set points.” Perhaps we should consider this in a similar way to how research shows the autonomic nervous system operates, where there can be coactivation, decoupled activation, and reciprocal activation” (Janssen & Bancroft, 2023, p. 133)
The simplified male sexual response model presented here focuses specifically on the dynamics leading up to the point of no return (PONR), rather than encompassing the full scope of the dual control model. The full zone theory (work in progress) integrates mathematical concepts from Blyuss & Kyrychko (2023) and other sources to address the dynamics of the thresholds. By concentrating on pre-PONR processes, this simplified version offers an elegant picture of submaximal threshold responses and the dynamics of factors that influence the arousal progression. This mathematical simplification allows for an intuitive, accessible, and economical analysis of the interplay between excitatory and inhibitory systems in male sexual arousal, particularly in the context of submaximal threshold response experiences.
In zone theory, everything is stochastic: the factors, the submaximal threshold spectrums, and the maximal threshold. By setting the equation as a fraction, the obstacle of the maximal threshold being non-constant is handled. Thus, ratios between the Arousal per PONR (t) and the maximum threshold (t) are used. Because it is not possible to assess the resulting value of all interactions of in ecosystem playing out at a psychological and physiological level, a psychometric is used to provide the total value for Arousal per PONR for each (t). As an aspect of zone theory, the ratio between one’s Arousal per PONR (t) and the maximum threshold, can be modeled by placing a mathematical expression of the dual control model over the maximum closeness-to-orgasm psychometric. For example, the Closeness to Orgasm Scale might be somewhat like the following:
Instructions: Please rate your experience on a scale from 1 to 10, where 1 represents no arousal and 10 represents the point of no return (PONR) or ejaculatory orgasm.
1. Arousal Level: 1 (No arousal) to 10 (Highest arousal without orgasm)
2. Genital Sensitivity: 1 (Normal sensitivity) to 10 (Extremely heightened sensitivity)
3. Muscle Tension: 1 (Completely relaxed) to 10 (Extreme tension in pelvic and surrounding muscles)
4. Breathing Rate: 1 (Normal breathing) to 10 (Rapid, shallow breathing)
5. Heart Rate: 1 (Resting heart rate) to 10 (Extremely elevated heart rate)
6. Mental Focus: 1 (Easily distracted) to 10 (Completely absorbed in the sensation)
7. Pleasure Intensity: 1 (Mild pleasure) to 10 (Intense, orgasm-like pleasure)
8. Urge to Ejaculate: 1 (No urge) to 10 (Overwhelming urge to ejaculate)
9. Involuntary Muscle Contractions: 1 (No contractions) to 10 (Strong, rhythmic contractions)
10. Perceived Proximity to Orgasm: 1 (Far from orgasm) to 10 (On the brink of orgasm/PONR)
Scoring: Calculate the average score across all items for an overall Closeness to Orgasm/Maximum score. Higher scores indicate greater proximity to maximal threshold response.
By entering the psychometric into the equation, one can solve for the factors. The factors for a given arousal need to be identified and their influence assessed. For instance, a psychometric of 3 would give 3/10 = (F + -F + F…)/10. One might identify multiple factors of high influence—feeling relaxed, comfort level, time of day, toy use, etc.—and weight them among a generated series of numbers for inhibitory and excitatory factors that sum to 3. Tools like regressions, psychometrics, and interviews can be used to assess weights for one’s model. Ideally, this method would be used in nanosexuality research, in which one specific sexual session is reversed engineered a combination of real-time data and retrospective analysis, using interdisciplinary approaches ad extremum with great contribution and self-case study from the participant researcher, plus subject matter expert augmentation.

The simplified zone theory model presented here suggests that maximal threshold responses—including antegrade ejaculation, retrograde ejaculation, prepubescent dry orgasm, inhibited ejaculation, and anejaculation—are not mutually exclusive from submaximal threshold responses such as NEOs. This framework allows for the possibility of experiencing both a maximal refractory “wet” orgasm (i.e., through retrograde ejaculation) and multiple dry non-refractory submaximal threshold responses with contractions. It is important to note that most prepubescent males typically do not achieve full climax due to insufficient and unsustained stimulation, meaning they often experience submaximal threshold responses rather than complete orgasms. Interestingly, when some adults (myself included) encounter submaximal responses for the first time, the sensation can be reminiscent of their masturbatory experiences during the latency period prior to the onset of ejaculation. Robin Fox (2004) likens prepubertal submaximal threshold response to tantric sex, an interesting connection. Historically, submaximal threshold response was prolonged in order to retain semen and participate in elaborate sexual ritual. Semen was believed to contain vital energy.
Submaximal Threshold Response in Practice
Males can experience submaximal threshold level responses through various methods, including relaxation techniques, start-stop masturbation, breathing exercises, slow-gentle stimulation, and Kegel exercises (Wibowo & Wassersug, 2016; Kothari, 1989; Hartman & Fithian, 1984; Robbins & Jensen, 1978). Researchers in the 1980s and 1990s believed specific techniques, particularly Kegels near the point of no return, were essential for achieving these responses (Keesling, 1994). However, this assumption was challenged by Whipple, Myers, and Komisaruk’s (1998) study, which documented a male who experienced multiple submaximal threshold responses with ejaculation without employing commonly cited techniques.
While the participant in Whipple, Myers, and Komisaruk’s (1998) study claimed to lack a refractory period, this assertion is not well-supported and contradicts existing research. Rather the participant had either had a very short refractory period or was experiencing multiple subthreshold level response with ejaculation called non-refractory ejaculatory responses. Nevertheless, the study demonstrates that submaximal threshold level response with ejaculation is possible without commonly cited techniques. It is suspected that the participant used slow masturbation and prolonged stimulation described by Hartman and Fithian (1984) based on the 30-minute session time. The study also suggests that the refractory period operates independently from ejaculation. The dual control model and fuzzy spectrum in zone theory indicate that infinite input combinations can lead to various arousal levels. This implies that specific techniques are not strictly necessary to achieve submaximal threshold responses, provided one remains within a certain range from the point of no return (PONR). However, some techniques may serve as more effective last-second excitatory or inhibitory factors, presenting an opportunity for future research to explore their relative efficacy.
It is important to note that not all individuals who practice edging or employ abovementioned techniques will experience submaximal threshold level responses commonly called the NEO with contractions and ruined orgasm (non-refractory ejaculatory response). Edging encompasses a spectrum of submaximal threshold responses, some of which overlap with NEOs. Given that penile response is threshold-specific, all techniques can be considered forms of edging, with the “edge” defined as 10/10 on the arousal scale, beyond which full climax and the refractory period occur in males..
Keesling (1994) popularized a numerical scale to describe proximity to the point of no return (PONR), such as “level 9 out of 10.” No metric has been made for consistency, so numbers are arbitrary when used in “how-tos.” Online forums reveal varied experiences (e.g., r/multiorgasmic), with some practitioners maintaining distance from the PONR, while others report intense sensations close to it, including involuntary contractions and multiple non-refractory ejaculations. The reported self-assessed numeric closeness are often varied on online forums, with some males reporting staying away from to the point of no return often, sometimes in an effort to practice semen retention. Others, such as myself, will go very close to the PONR feeling almost constant ejaculatory inevitability and peak penile pleasure, with numerous involuntary anal contractions, multiple non-refractory ejaculations, or sensations that wax and wane without contractions.
Although Robbins and Jensen (1978) emphasize that multiple orgasmic responses should not be confused with a controlled, prolonged plateau phase, they employ an orgasm-by-contraction typology to distinguish NEOs from non-NEOs. However, the boundary between submaximal threshold responses can be fuzzy, as similar sensations can occur without contractions, leading to debates about what constitutes a NEO. Davidson (1980) further questions whether muscle contractions are essential for the orgasmic experience, encompassing both submaximal and maximal threshold responses, stating that “[r]elevant information has recently become available from observations on “multiorgasmic” men…. there is a question about the quality and intensity of the preejaculatory orgasms, and they have been described as “miniorgasms” in a popular magazine (Petersen, 1977)” (Davidson, 1980, p. 301-302). Reports from online communities such as r/multiorgasmic suggest that the intensity of NEOs can vary significantly. Some NEOs are reported to surpass maximal responses in duration, intensity, and other dimensions, while others are described as relatively mild in comparison. This variability in experience highlights the complex nature of submaximal threshold sexual responses in males. The subjective value of these experiences also varies among individuals. Some practitioners report preferring multiple NEOs over a single maximal climax, or even over multiple maximal releases spread throughout the day. This preference may be due to the cumulative pleasure derived from numerous submaximal threshold experiences, the absence of a refractory period allowing for prolonged arousal, or other factors unique to NEOs. This diversity in experience suggests that traditional models of male sexual response may not fully capture the range of pleasurable experiences available to men who explore these techniques.
Current scientific consensus maintains that adult males invariably experience a refractory period following a maximal orgasm response, despite isolated claims to the contrary. The study by Whipple, Myers, & Komisaruk (1998), which featured a male participant reporting no refractory period, provides insufficient evidence to challenge this established understanding. Observations from adult content platforms showcase males achieving numerous ejaculations within brief time frames (e.g., 10 minutes). However, these instances typically involve techniques that keep arousal levels close to the point of no return (PONR) without fully crossing it, rather than a true absence of a refractory period. Historical data from Kinsey et al. (1948) suggested that prepubescent males might experience multiple climaxes with minimal or no refractory period. However, for good reason, ethical considerations prevent modern scientific verification of these claims in laboratory settings. Given the current body of evidence, Masters and Johnson’s (1966) assertion remains valid: adult males inevitably experience a refractory period following a full climax. This refractory period should be considered an integral component of the maximal orgasm response in males, distinguishing it from submaximal threshold experiences that lack this feature.
The Anal Contraction Reflex
The orgasm reflex, like other physiological reflexes, is defined as an involuntary motor response triggered by a stimulus, which may or may not be consciously perceived. This response follows a fixed reflex arc and is generally stereotyped, meaning it cannot be altered or adapted to specific circumstances.
The reflex arc consists of five key components (Pedroso, 2008):
- A receptor (e.g., sensory organ or nerve endings)
- A sensory or afferent neuron
- An internuncial neuron in the central nervous system
- A motor or efferent neuron
- An effector organ (muscle, gland, or blood vessel)
The orgasm reflex is quasi-threshold dependent. This means that its activation threshold is not fixed. It is influenced by both psychological and physiological factors. Some individuals have higher orgasm thresholds than others, as show in Schnarch’s (1991) economic model of sexual response. For instance, just as a physician might not strike the patella with sufficient force to elicit the knee-jerk reflex, the orgasm reflex can be modulated by various factors. Individuals can consciously influence the threshold for triggering the orgasm reflex. This can be done by flexing surrounding muscles or through mental focus, which can either inhibit or facilitate the induction of the reflex. This ability to modulate the reflex threshold demonstrates the complex interplay between voluntary control and involuntary physiological responses in human sexual function.
The NEO and the maximal response at the PONR both involve the same external sphincter reflex, highlighting the physiological similarities between these experiences. Traditionally, ejaculation and orgasm are divided into two phases: the emission phase (involving the vas deferens, seminal vesicles, and prostate gland) and the expulsion phase (involving the external urethral and anal sphincter, pubococcygeus, bulbospongiosus, ischiocavernosus, and perineal muscles). NEOs demonstrate that the expulsion phase contractions can occur independently of the emission phase. Another submaximal threshold phenomenon, the non-refractory ejaculatory orgasm (also known as a ruined orgasm), further complicates our understanding. This experience shows that ejaculation alone does not necessarily trigger the male refractory period. It suggests that both the emission and expulsion phases can occur to some extent without inducing a refractory period, implying a separate mechanism for the refractory response distinct from semen emission and pelvic floor contractions. It is possible that the throbbing of the bulbospongiosus muscle in the penis is similar in both NEOs and refractory climaxes, while contractions of the external anal sphincter may vary individually. However, to date, this specific comparison has not been empirically measured. These observations challenge traditional models of male sexual response and highlight the need for further research to more adequately understand the mechanisms underlying various orgasmic experiences and the refractory period in males.
Literature Review
The idea that contractions for nontermative orgasm and termative orgasm are similar and different does have scholarly support. Davidson (1980) talked with B. Campbell who studied multiorgasmic men and noted that the cardiovascular and respiratory changes and the contractions of the muscles of the pelvic floor recorded from intra-anal transducers during non-ejaculatory orgasms were not different from those recorded during normal male ejaculation. However, B. Campbell never published any of this data. Carmichael et al.’s (1994, p. 76) results differ from previous reports of lack of differences in cardiovascular, respiratory, and pelvic muscle contraction data between non ejaculatory and ejaculatory orgasms, also noting systolic blood pressure and electromyographical amplitude that were significantly higher during orgasms without ejaculation than those without in their multiorgasmic male participant. Unfortunately, Carmichael et al. (1994) never published the graphical data either.
What causes the contractions?
I will quote Davidson’s (1980) answer, which considers the case of the female when considering male multiple non-ejaculatory responses. The quotation also serves as a good leeway into the next session: “Are contractions a necessary dimension of orgasm?”
“One view (Sherfey, 1972, p. 74) is that orgasm is physiologically triggered in both sexes by a stretch reflex mechanism in which the stimulus comes from vasocongestive distension in the genital tissues and that the response is vigorous contraction of the perineal-genital muscles, which expel blood trapped in the venous plexuses. This author believes that the expulsion of blood “creates” the orgasmic sensations. Masters stated that the relevant sensations in the male are derived from seminal expulsion (Masters & Johnson, 1966, p. 212), while also holding (Masters, 1960) that “actual orgasmic experiences are initiated in both sexes by similar muscle components.” Yet, in describing the female orgasmic experience, Masters and Johnson (1966) delineated three stages: first a sensation of “stoppage” (akin to “bearing down” in labor), then a flow of warmth from the pelvis over the body, and then contractions leading to throbbing sensations. The first two stages of the female orgasmic experience therefore precede the pelvic muscle contractions (which expel semen in the male). In fact, these authors stated explicitly that the “sensation” of orgasm begins 2-4 sec before “she responds physiologically” (p. 118). They further remarked that in subjects for whom the increase in tension is great, there is an initial muscle spasm before the rhythmic contractions, which “parallels the subjective report of orgasm.” This spasm is, however, stated to occur during the third stage. It is compared to the first stage of male ejaculation 2-4 sec before the appearance of semen at the urethral meatus (see below). This stage carries with it the sensation of ejaculatory inevitability rather than the actual experience of orgasm, which can be delayed beyond this stage. Obviously, there is no clarity, not only about what actually causes orgasm but also about when it begins or ends, that is, which coital events may be defined as truly orgasmic (see also Kinsey et ai., 1953, pp. 627-628.) If several clinical reports that claim that female orgasm can occur in the absence of contractions of vaginal and pelvic floor muscles (Singer, 1973, p. 66ff) are to be believed, the present emphasis on these contractions would seem inappropriate. This phenomenon has not, however, been demonstrated under controlled conditions. If perception of pelvic muscular activity is essential for orgasm, we might ask what are the intervening mechanisms between these contractions and the experience? What role is played by direct perception of other muscular, vascular, respiratory, and/or other overt physiological events? And what about the more covert physiological processes of which we may not be consciously aware? These kinds of questions can, of course, be asked about any emotional experience but seldom with the immediacy and the richness of specific physical and experiential events as in orgasm” (Davidson, 1980, p. 300-301).
Are contractions a necessary dimension of orgasm?
Use of contractions as a litmus test for orgasms has a dark history related to female frigidity. As Bergler (1944) put it, “a man can be deceived by a clever woman in many things—in love, sensitivity, sexual interest, pleasure in intercourse. In only one thing is she helpless—the production of involuntary contractions” (p. 379).” Today, the same litmus test is used for submaximal threshold responses, like NEOs. In “Electrode” by Dani Ploeger (2011), Ploeger stood in a room before a projector screen and tried to replicate slowed-down sphincter muscle contraction patterns observed in an anonymous male subject during masturbation and orgasm. The performance serves as a critique of societal and scientific perceptions of orgasm, challenging traditional notions of authenticity and embodiment. Critics of the Lioness Smart Vibrator, a vibrator that detects contractions, see it as part of a relic of neoliberal biomedical models of quantification (Kressbach, 2024).
The paradox of NEOs without contractions lies in how an orgasm can occur without the typical orgasm reflex. Literature on females frequently describes orgasms without contractions, and many porn videos claiming “real female orgasms” show models reporting orgasms without visible contractions. In fact, the subreddit r/orgasmiccontractions uses visible anal contractions to differentiate “real” orgasms from “fake” ones, or rather, maximal and higher submaximal responses from lower ones. Faked penile, vaginal, and anal contractions can be considered a subset of fake orgasm typology. However, not all mimicry is deceitful; it can be enjoyable and embodied (Frith, 2018). Anal wink pornography can potentially mimic contractions convincingly, especially without a probe to measure contraction parameters. Research indicates that voluntary mimicked orgasms can be distinguished from involuntary ones using rectal probes, at least in females (van Netten et al., 2008), but just observing the anus winking externally might not suffice for detecting orgasms. Powers (1992) describes this response as a plateau phase orgasm, noting that males can also experience it. This suggests that male and female submaximal responses can be quite similar to the point where orgasms without the contraction reflex but with other orgasm markers are still considered orgasms but not climaxes.
Why does it matter when the NEO and maximal response can share almost 90% of Mah and Binik’s (2001) dimensions? In practice, it does not matter unless the individual has a specific interest in contractions. For researchers, having a distinct contraction profile that distinguishes a NEO from a refractory ejaculatory orgasm would provide an objective way to differentiate these types and assess whether there are males who truly lack a refractory period and can experience maximal responses within seconds or less than a minute apart, aligning with the strictest definitions of multiorgasmia in females (See Gérard et al., 2021.). Although unverified, teenage males and prepubescent males might have maximal orgasms at an inter-orgasm interval comparable to maximal threshold orgasmic response in females under strict definitions, or at least within a couple minutes of each other owing to a short relative or absolute refractory period (Kinsey et al., 1948).
Bohlen et al. (1982) only found that female reported an orgasm without contractions. However, males in r/multiorgasmic and other communities have also reported penile response without contractions. It is especially interesting to note in this context that Bohlen et al. (1982) stated that although two of their 11 subjects did not show distinct muscular evidence of orgasm they were not prepared to conclude that “physiological characteristics are more valid than self-reported perceptions for identifying orgasm…. At least until more data are collected.… we will continue our analyses of physiological changes based on subject’s self-defined orgasms” (p. 791). Powers (1992) has a typology for this: “Plateau orgasm was conceived because orgasm (general definition) may occur during a physiological state corresponding to the excitement phase (especially during a “plateau”) in the sexual response sequence. For example, Hite (1976) found women who reported orgasm without rhythmic vaginal contractions or intense genital sensations. Hite referred to this type of experience as “emotional orgasm.” Bohlen et al. (1982a; 1982b) found some female subjects who signaled orgasm, but whose records failed to show any rhythmic contractions. Excitement-phase plateaus may be interpreted as orgasmic or, to use Kline-Graber and Graber’s (1975) term, “a pre-orgasmic phenomenon.” Followers of Tantrism engage in erotic rites which involve prolonged sexual intercourse without male ejaculation. It is believed that by sustaining a plateau-level state of meditative-coital ecstasy, the practitioners may induce spiritual enlightenment (Tannahill, 1980). Plateau orgasm is characterized by a random contraction pattern. It is nonterminative and may be involved in reported multiorgasmic experiences” (p. 55). Submaximal threshold response near or close to the PONR of no return can also trigger the full or a portion of the orgasm contraction reflex without ejaculation and without triggering the refractory mechanism, meaning that there are three mechanisms at play: orgasm, ejaculation, and the refractory mechanism, which is yet to be understood.
My view much aligns with neuroscientist Nicole Prause. In a Vice interview, Nicole Prause expressed a dissenting opinion: no contractions, no orgasm. In response to what some females describe as mini orgasms, Nicole Prause is skeptical, believing that ““Mini orgasmic” isn’t a term recognized by scientists…. Prause believes Masters’ and Johnson’s data show peaks in arousal that stop short of orgasm. “We have a few data examples now of people—especially women—get into a brain state associated with reduced cognitive control that appears to be necessary prior to orgasm, then drop back to a ‘trying hard’ engaged state increasing sexual arousal,” she says. “The pushes are not associated with any contractions defined physiologically as climax’” (Weiss, 2018, para. 8). In another interview, Prause noted that “If orgasm marked the height of pleasure, you’d think chill waves would keep rising. But they don’t; they drop. That makes orgasm not an off-switch but more like a “back on” switch, pulling you out of the trance that preceded it. For Prause, this suggests that the best part of sex—the thing that keeps you coming back for more—is not the orgasm but the part leading up to it, what she refers to as a high-pleasure state and the kids call “edging,” when you deliberately delay orgasm to make sex last longer, potentially making the eventual orgasm stronger. Your takeaway: If she doesn’t have an orgasm and insists she’s fine, she might actually mean it. “Orgasm isn’t magic,” says Prause. “Not that it’s not reinforcing, but everything before it is also reinforcing.” Some women may even confuse high arousal for orgasm and still report satisfaction. During her research, Prause found many of the women reporting orgasm did not have the pelvic contractions traditionally used to define it. At first she thought the anal probe—which senses the contractions—was faulty. But as the trend persisted, she realized that these women were not experiencing orgasms, even though they believed they were. (She did not see this in men.) Komisaruk and others maintain that women do know when they’re having an orgasm and that you don’t have to count contractions to prove it. (Georgiadis had a finding similar to Prause’s; for many of his female subjects, the anal probe’s signal was “messy,” lacking the clear pattern seen in men.) Even Prause’s male research partner was skeptical. “I think it’s funny that I’m the only woman in this bunch,” Prause says, “and I’m like, ‘Women are terrible at telling orgasms.’” All this made me think about my orgasm in the little room, which felt great—and, yes, was confirmed by anal probe data. But is the release the thing? Maybe the wondrous feeling I’ve been enjoying for 15 years is actually the high-pleasure state and not orgasm at all. Maybe it’s the path to climax we should’ve been pursuing all this time” (Covert, 2017, n.p.). I find it ironic that in the case of the NEO the same discussion occurs.
Furthermore, when it comes to multiple orgasms with claims of females having 134 orgasms in an hour (e.g., Hartman & Fithian, 1984; measured by heart rate), Prause’s research suggests that female figures are highly inflated and those of males are far underrepresented. “For women, it doesn’t help that the popular press is rife with misinformation. Women cannot have an hourlong orgasm, Prause points out, despite what the latest magazine cover might have you believe” (Konnikova, 2015, p. 20). In an interview with Hone Health (2024), Prause described testing a group of women at one point. Their only job was to press a button when their orgasm started and when it finished. About half of the women pressed the button, but there were no contractions. Prause checked that the probe did not fall out and checked the probe to see if something was wrong with the probe, but they were functioning. Prause believes that this reflects an education issue since they are not taught that they are supposed to have contractions so maybe they just call pleasurable instances orgasms. Prause had a few women in that were very vocal about having an amazing capability of multiple orgasms; They claim they had 40 in a session or 5 at one time; those were the women not having contractions. Very few studies look at physiological response but rather brain imaging (Hone Health, 2024). Perhaps this is an artifact of expanded orgasm typology.
When interviewed by Gilmour (2019), Prause noted that “We always tell this story that the idea of multiple orgasms in men [and people who have penises] is quite rare,” Dr Prause says. “And I don’t think that’s the case anymore. Mostly because women who say they have multiple orgasms, we find they’re not actually having contractions. My sense is these women are having some kind of pleasurable experience – I don’t think they’re lying to us or deceiving the trials – but they’re not having actual physical climax.” Currently, there is no scientific definition for multiple orgasms. “Something we’re speculating about is those who seem to have the longest latency between those multiple orgasms may be having separate events,” Dr Prause explains. “When there’s five to 10 minutes between orgasms and contractions, I would say they are pretty separate events.” Dr Prause also says those advice articles you’ll see on “How to give a woman five orgasms in three minutes” are just plain BS. “I see those, and I’m doing the math and knowing that isn’t even possible.” But, she wants to make clear that she’s not in the business of telling anyone the orgasms they have don’t count. “From the perspective of women and orgasms, I’m happy to describe how physiologists define these things. But if you think you’re having them and you’re having fun, I don’t want to tell you that’s not good enough. I realize there’s a high risk of that with this kind of data. I don’t want to yuck anyone’s yum.” (paras. 15). Given zone theory, some responses in females that do show some contraction pattern might well be submaximal threshold level response, warranting future research that can help differentiate these potential experiences, which some female edgers I spoke with about zone theory reported having.
My friend responded to my empirical physiologist view: “I just imagine you walking on a Betty Dodson group orgasm session back in the day and arguing that these are not real orgasms. “No wait, stop, you people don’t understand! You do know these are not real orgasms, right ? * waves around lab report * You’d be chased out of the room while being bonked over the head with Hitachi wands. 🤷♂️ It’s the whole idea that “technically right” is the best kind of “right”. You can’t say that 5 orgasms in 3 minutes is bullshit, then in the next sentence say that you’re not tying to say these “pseudo-Os” do not count.
Perhaps a fuzzy set orgasmic dimensions could be a solution between this orgasmic and nonorgasmic dichotomy. It could split into degrees of orgasmic experiences and have contractions to indicate that degree. For example, one might not feel quivering, pulsating, throbbing and rhythmic sensations with release of tension (relieving, releasing, erupting, exploding), but might experience other dimensions to some extent through the time series of a session, including Sensory aspects—spreading sensations (flowing, spreading, radiating), whole-body involvement (trembling shuddering), ejaculatory sensations (oozing, spurting, shooting), buildup of tension (rising, building, swelling), thermal sensations (cool, warm, hot), and miscellaneous (tickling, tingling, flushing), evaluative aspects—feeling of inevitability (inevitable), temporal evaluation (quick, long, unending), intensity (mild, moderate, intense, powerful), physical effects (relaxing, engulfing, exhausting), depth (deep, full, complete), global pleasure (pleasant, enjoyable, pleasurable, incredible), sensual pleasure (soothing, sweet, sensual, exquisite), satisfaction (satisfying, gratifying, fulfilling, cathartic), excitement (exhilarating, exciting, wild), and affective aspects—emotional intimacy (close, loving), joy-peacefulness (peaceful, blissful, tender), joy-elation (elated, ecstatic, euphoric, rapturous, passionate), emotional-excitation (abandon, uncontrolled), emotional fusion (immersing, merging, unifying), unreality (light-headed, dizzy), lack of awareness of surround (detached, oblivious, unreal), suspension (suspended, soaring), and miscellaneous (melting, vulnerable). Focusing on what is present and experienced versus what is not experienced validates rather than invalidates an experience.
In terms of zone theory, females tend to have higher orgasmic thresholds than males (Schnarch, 1991), meaning that they have more of a range in which to have subthreshold level experience. Perhaps this is why they tend to report a lot of orgasms that fit within subthreshold level response. See the preliminary figure for female zone theory:
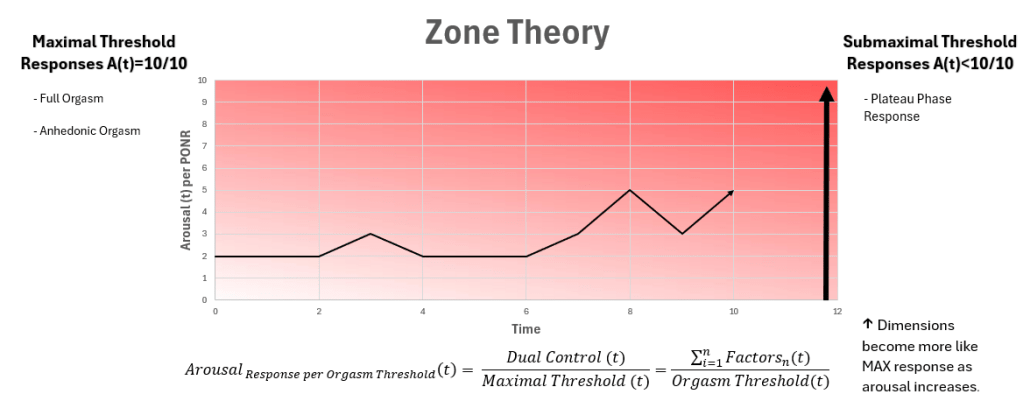
There is certainly a maximal and submaximal threshold response. However, individuals tend to not like when an orgasm is not considered an orgasm. In such cases, one might not classify by orgasm and non-orgasm but use fuzzy set of response dimensions, which when examined can help to determine maximal and submaximal threshold response. As one approaches the maximal threshold, there is a tendency for more dimensions of the ejaculatory orgasm to be experienced, like partial non-refractory ejaculations and anal contractions, which make them objective correlates of the subthreshold response called the NEO or non-refractory ejaculatory orgasm in males. Likewise, for females, there is a tendency for more dimensions of the ejaculatory orgasm to be experienced, although objective measures of submaximal threshold response, like those in the male, are unknown. The presence of a refractory period can differentiate the NEO and non-refractory ejaculatory orgasm. There is not enough data to say whether contractions alone can singularly differentiate between a submaximal threshold response like the NEO and a maximal threshold refractory response.
Methods
All raw or graphical data on anal contractions during non-ejaculatory and refractory orgasms at the point of no return were extracted from studies that used anal metrics to study orgasm. This information included anal photoplethysmography, pneumatic anal probes, and data from the Lioness Smart Vibrator, primarily used by females but also used by males who shared their data via phones. Caution was exercised when reviewing Lioness data, as the sensor is prone to user artifacts and orientation issues, making the data unreliable, often with inflated orgasm counts (e.g., 200 orgasms in 10 minutes). For comparison, all refractory orgasms at the PONR from the literature were included.
Data
A search for anal photoplethysmography, pneumatic anal probe, and Lioness Smart Vibrator data resulted in the following graphs and table. No raw data was published for any study. The graphs are sorted by refractory orgasms at the PONR. Across all studies and online sources, where the Lioness vibrator (primarily used vaginally by females) was used by males, data for NEOs was published for only three individuals. Robbins and Jensen (1978) had 13 participants but published anal probe data for only one. Carmichael et al. (1994) had only one participant who experienced multiple submaximal threshold responses, labelled as multiple orgasms. Rudolf Arnold (2020) published data solely on himself as part of his orgasmic dancing performance with a sonified anal probe, with the objective of making anal contractions musical. Taken collectively, with data from only 3 people across studies in the last 50 years, no generalizations can be made.
Maximal Threshold Responses (Refractory Ejaculatory Orgasm at PONR)
From Bohlen et al. (1980)
From Bohlen et al. (1980)

From Bohlen et al. (1980)
From Bohlen et al. (1980)
From Bohlen et al. (1980)
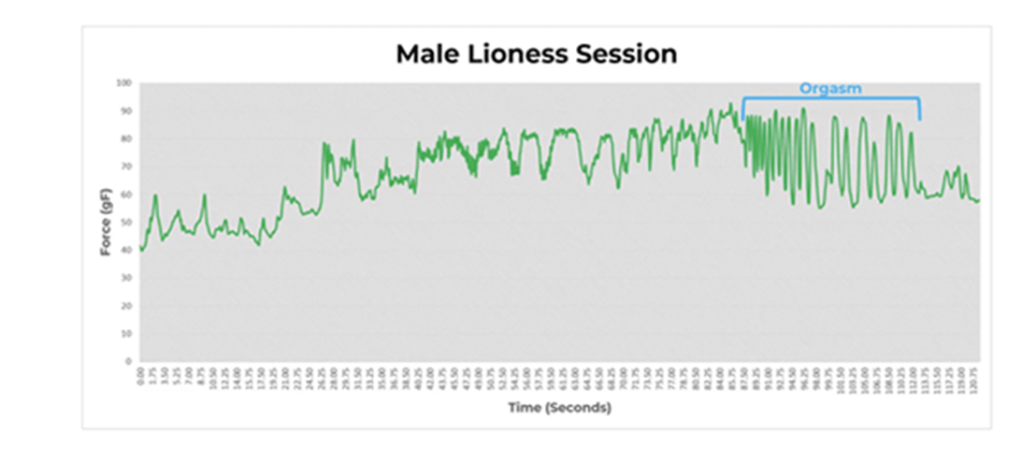
From (Lee, 2019)
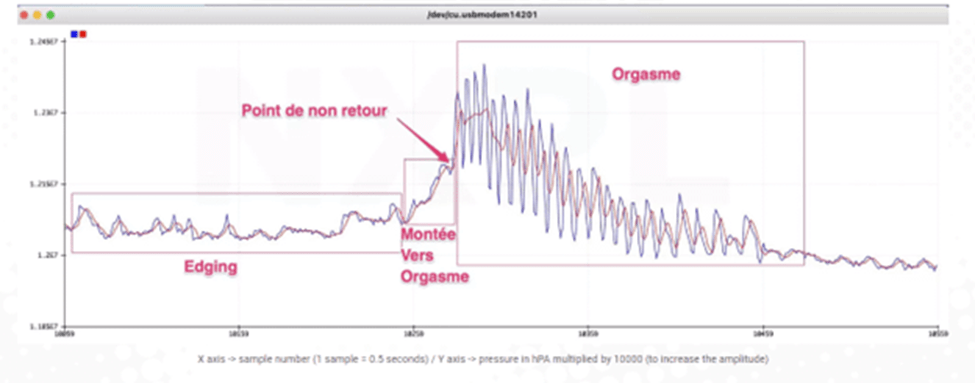
From (Nouveaux Plaisirs, 2021)
Submaximal Threshold Level Responses (Non-Ejaculatory Orgasms)
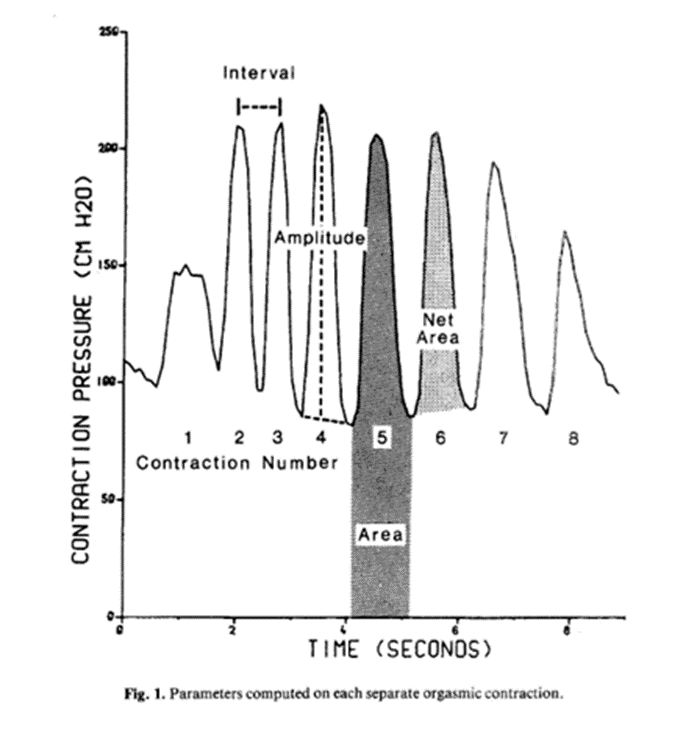
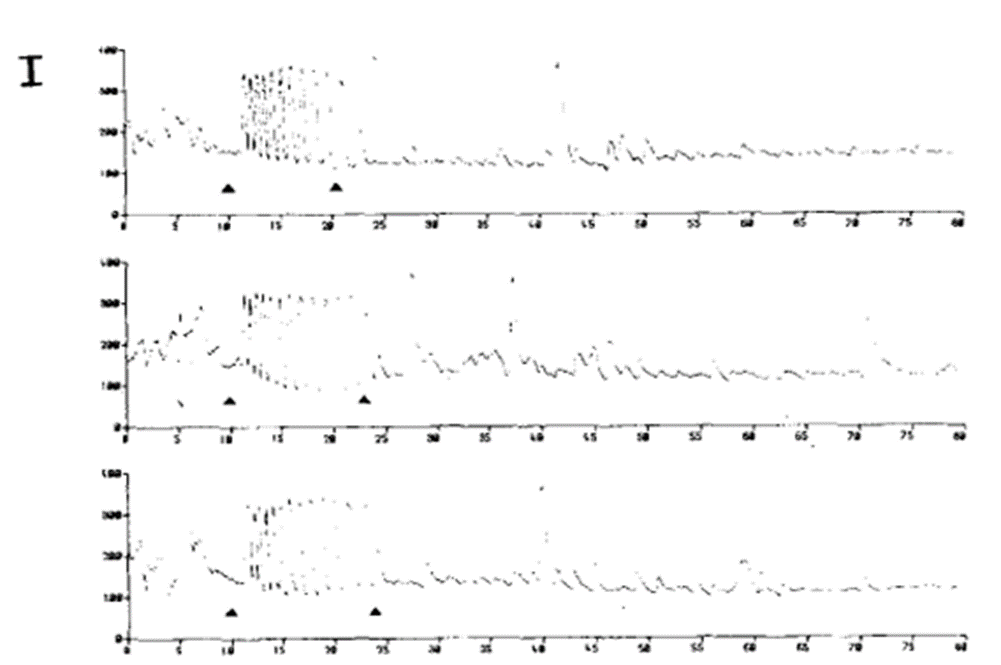
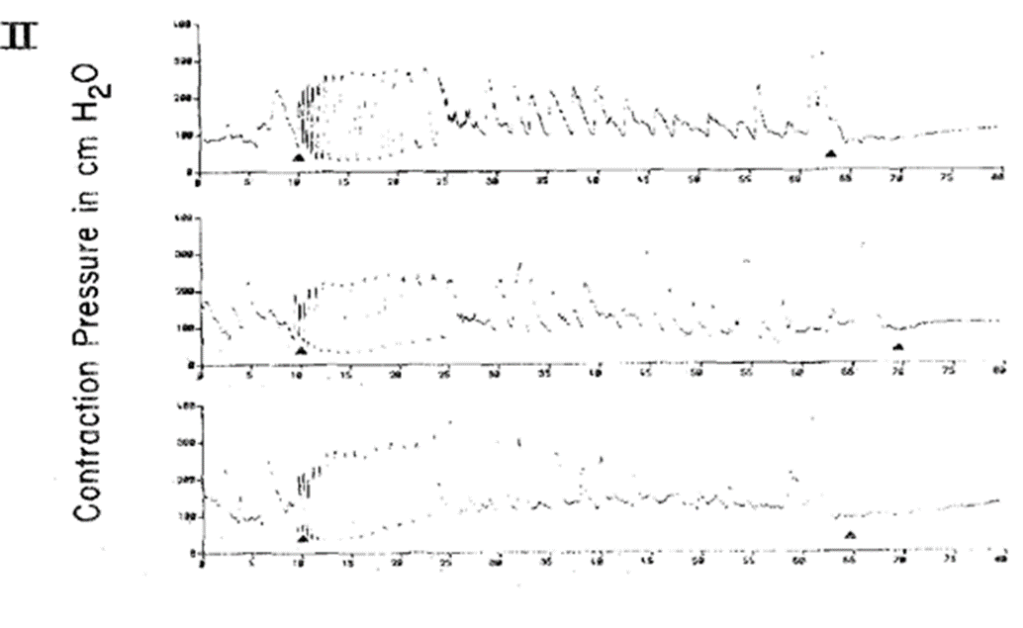
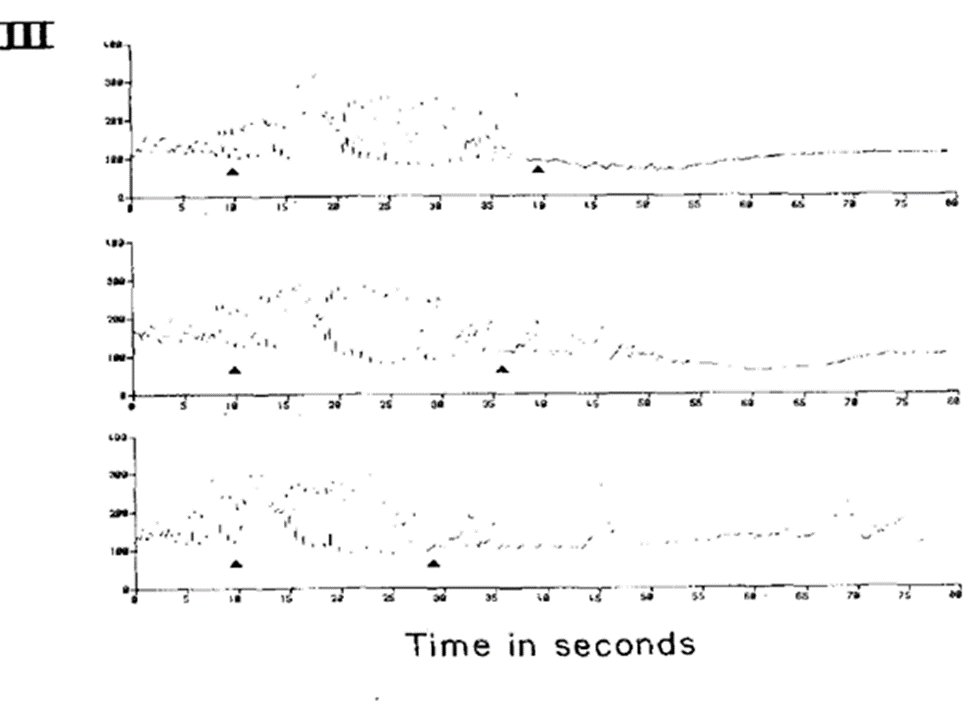
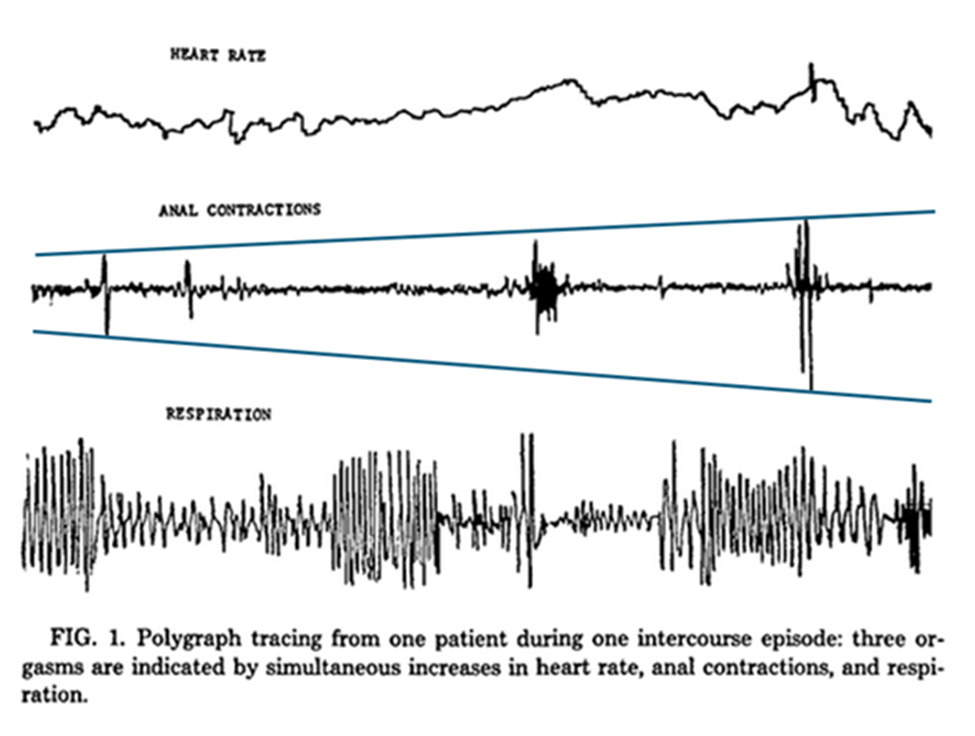
The polygraph tracings (Figure 1) show three orgasms of a series in which ejaculation accompanied the last recorded orgasm.
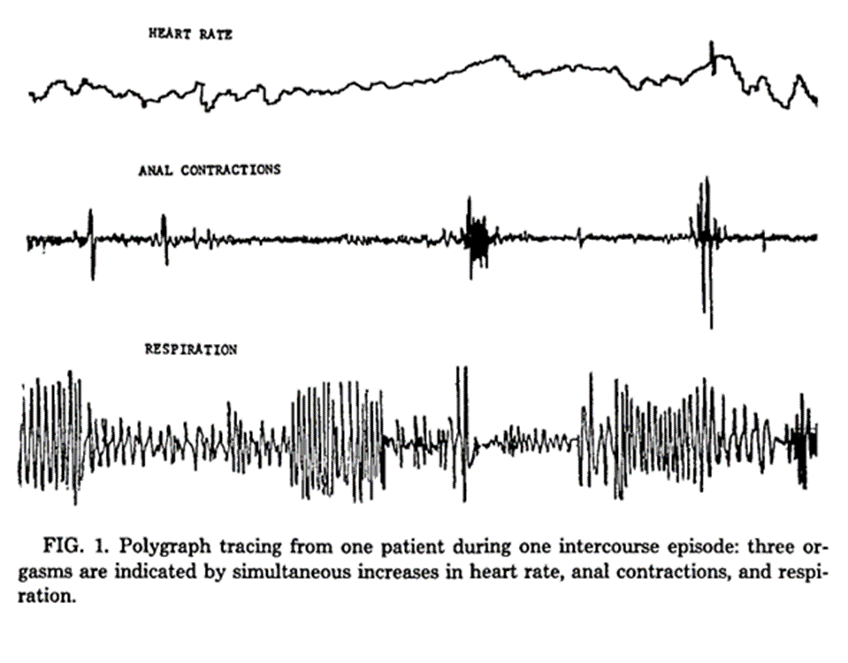
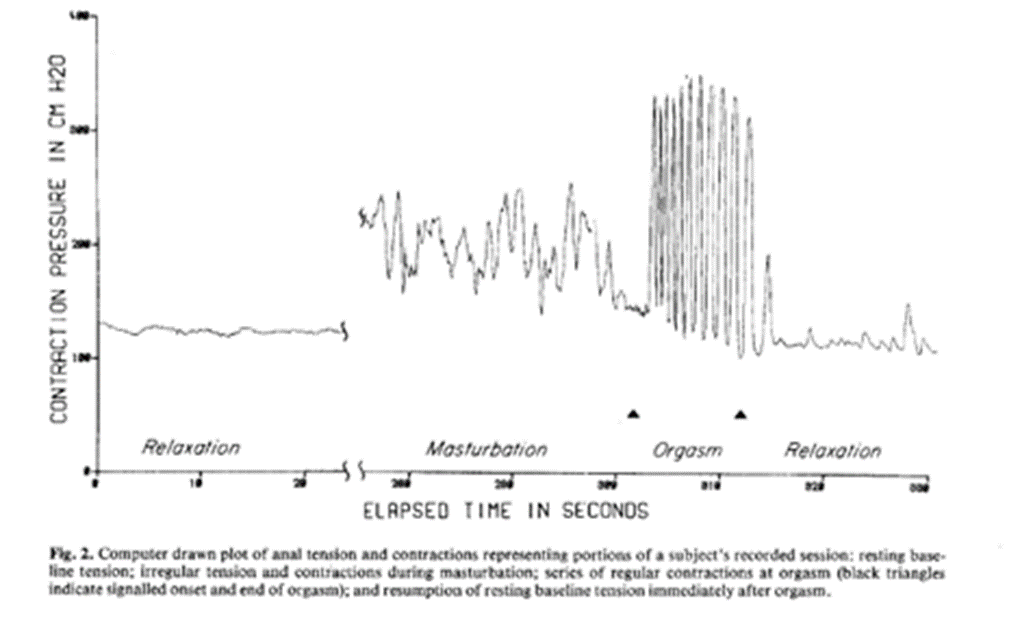
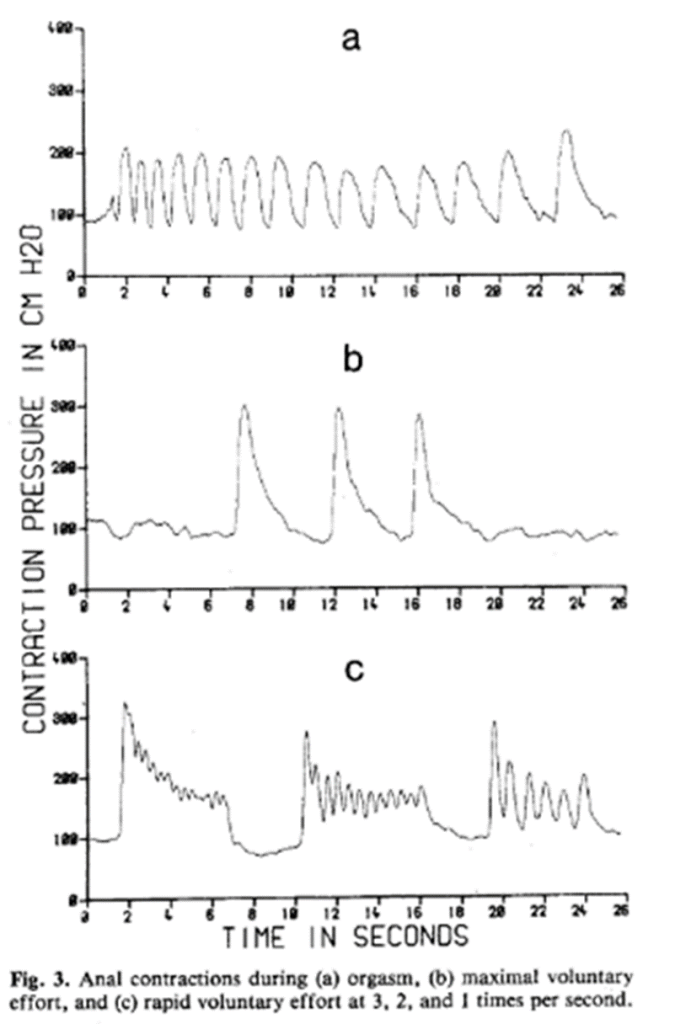
From (Robbins & Jensen, 1978)
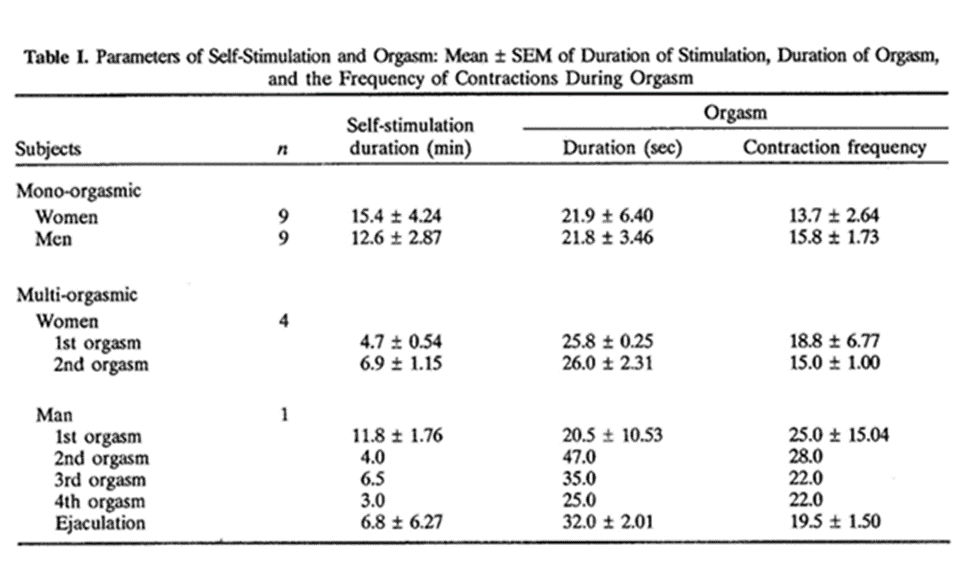
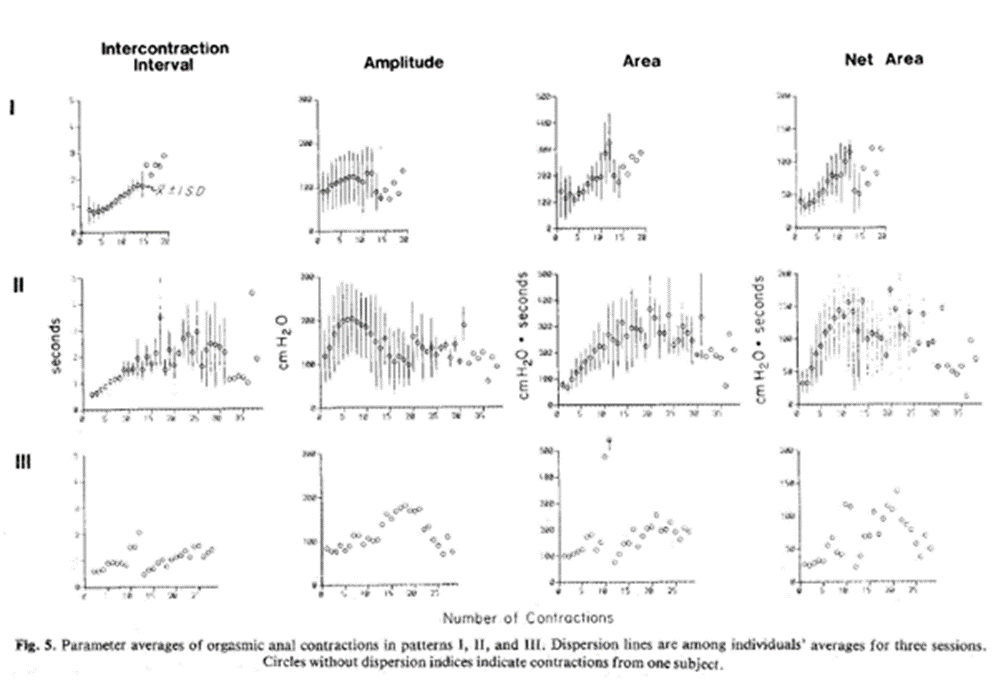
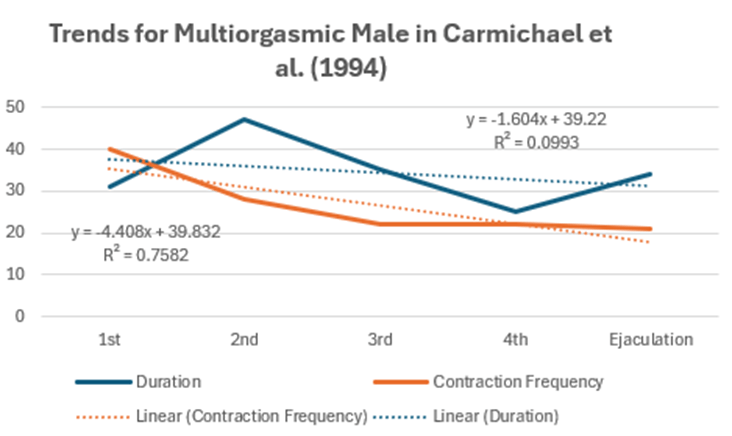
From (Carmichael et al., 1994)
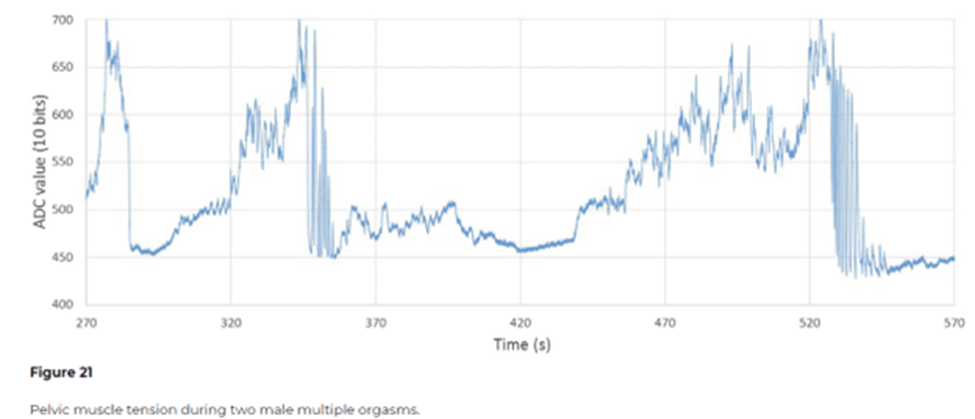
From (Arnold, 2020)
Data Analysis
This data analysis section examines graphical representations derived from various physiological measurement techniques, including anal photoplethysmography, pneumatic anal probes, and the Lioness Smart Vibrator. While the dataset is limited and primarily visual in nature, it offers valuable insights into contraction patterns observed during NEOs and refractory phenomena at the point of no return (PONR).
The data for submaximal threshold responses (NEOs) was sourced from three key studies:
- Robbins and Jensen (1978)
- Carmichael et al. (1994)
- Arnold (2020)
Importantly, all NEO data in these studies included same-person maximal threshold response data, allowing for more meaningful comparisons than those made between different individuals.
Additional contraction data for maximal threshold responses was obtained from:
- Bohlen et al. (1980)
- Lee (2019)
- Nouveaux Plaisirs (2021)
Robbins and Jensen’s (1978) graphical data, while lacking axis labels, provides visually discernible differences in contraction patterns. The crest and trough heights, as well as their durations, show noticeable variations not only between two separate instances of NEOs but also when compared to the final ejaculatory event. This variability in contraction profiles suggests that submaximal threshold responses can differ from one another, as well as from the maximal climax. Such observations indicate that NEOs may not be uniform experiences, but rather a range of contraction profiles that can vary in intensity and character.
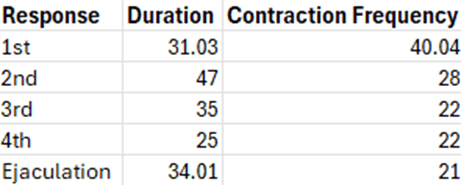
Carmichael et al.’s (1994) study presents some limitations in its data presentation. The criteria for determining contraction intervals and orgasm cessation in the contraction data are not clearly defined, and the actual contraction waveforms are not provided. In contrast to Robbins and Jensen’s (1978) data, this study reports higher contraction frequencies in NEOs, with a downward slope towards ejaculation. The use of a light sensor may have introduced artifacts into the data. Moreover, the absence of published graphs from the multi-orgasmic male participant limits comprehensive analysis. It is unknown what the contractions actually looked like. The tabulated data indicates that NEO durations exceeded their frequency durations. Anecdotal subjective reports, including my own, suggest that NEO contractions may be shorter than ejaculatory orgasms, with other dimensions varying widely. The sensational difference between NEOs with and without contractions is reported to be minimal, with arousal deviations occurring in both cases. They report that their personal experience with NEOs involves shorter contractions compared to ejaculatory orgasms, while other dimensions vary considerably, ranging from less intense to more intense than ejaculatory orgasms, especially when experience frequently for up to an hour. Contrary to some reports suggesting discrete responses are more powerful than continuous ones (Hartman & Fithian, 1984), multiple submaximal threshold responses had for a long period of time can be subjectively rated as more intense than single instances. Each NEO, whether discrete or continuous, possesses a unique profile in terms of duration and intensity. Carmichel et al.’s (1994, p. 76) adds that “interestingly enough, the duration of orgasm was not correlated with positive affect or subjective magnitude. Thus, brief orgasms were reported just as pleasurable, satisfying, and intense as longer orgasms” (p. 76). The individual variability in NEO experiences challenges generalizations about the relative intensity of different submaximal threshold responses.
Taking the maximal of the ranges, subjective report was as follows:
Of the studies, Arnold’s (2020) study provides the highest quality data among the reviewed studies. The data reveals similarities in contraction patterns between the first submaximal threshold response and the orgasm at the PONR, though the former shows less regularity. A notable feature is the more stable baseline following the orgasm at the PONR, which could potentially serve as a correlate of orgasm. It is important to note that Arnold was dancing during the session, which introduces a potential confounding factor. The more stable line after the PONR orgasm might be attributed to reduced movement as relaxation sets in and a state deviation occurs. The precise effect of dancing on the contraction patterns remains unknown. Despite this limitation, the orgasmic events are distinctly identifiable from artifacts caused by dancing movements.
To facilitate further analysis, the graphical data was digitized using WebPlotDigitizer software, allowing for approximate numerical representation of the original data. This digitized data provides a basis for more detailed quantitative analysis. It can be viewed here. https://docs.google.com/spreadsheets/d/1UzxhXHj3yw4E-ARD3ogktHtTEfw_OJe_/edit?usp=sharing&ouid=110245894519320091781&rtpof=true&sd=true
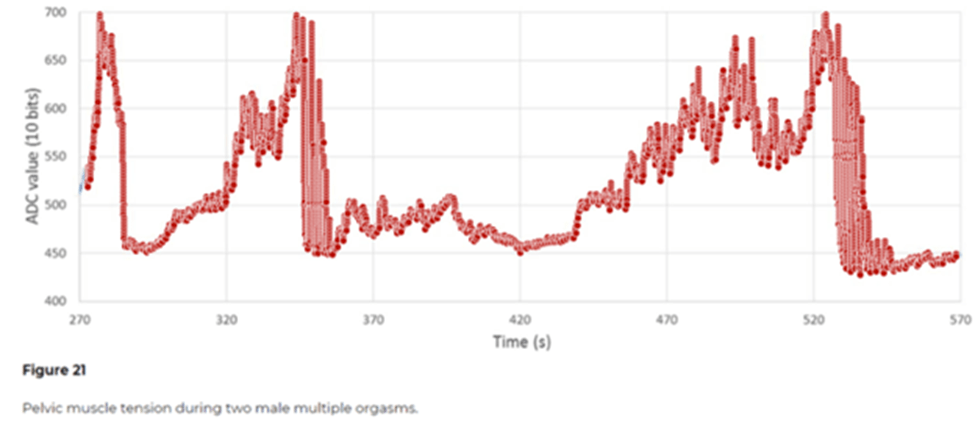
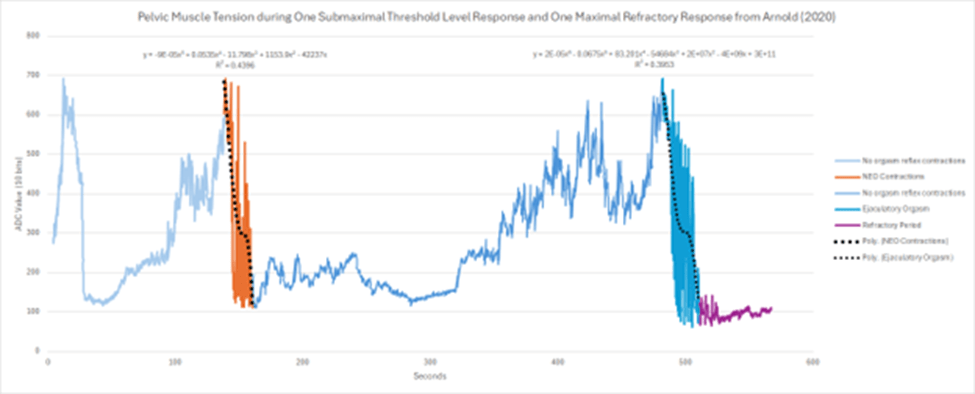
The initial contraction set, highlighted in orange, represents a NEO or submaximal threshold response. Both the NEO and the ejaculatory orgasm at the point of no return (PONR) exhibit peak contractions around 700 ADC, with the ejaculatory orgasm showing slightly lower values, up to 50 ADC less. The NEO displays greater irregularity in its contraction pattern and fewer crests compared to the orgasm at the PONR. The NEO contractions span approximately 21 seconds, from the 139-second to the 160-second mark. In contrast, the refractory ejaculatory orgasm contractions last about 28 seconds, occurring between the 482-second and 510-second marks. This represents a 7-second difference in duration between the NEO and the refractory ejaculatory orgasm. Despite this difference, the NEO’s duration falls within the range expected for refractory ejaculatory orgasms as reported by Bohlen et al. (1980; 1982):
- Type 1: a simple series of regular contractions
Male (6.4 – 31.3 sec.; 8-18 contractions) | Female (7.4-15.6 sec.; 8-15 contractions)
- Type 2: regular series and then irregular contractions
Male (20.1-56.1 sec.; 13-33 contractions) | Female (17.7-107.6 sec.; 9-34 contractions)
- Type 3: Preliminary contractions before the series of regular contraction in midorgasm
Male (25 sec.; no dispursion indices) | Female (unknown, unknown)
- Type 4: no contractions although orgasm was reported
Male (N/A) | Female (24.4, N/A)
This similarity in length suggests a potential physiological equivalence between NEOs and full climax experiences, at least in terms of contraction duration. A good indicator between the NEO and refractory ejaculatory orgasm is the after period. The pelvic floor tension is less in the period following the conventional orgasm than the NEO, which corresponds to the degree of post-response deviation. These observations highlight both the similarities and differences between NEOs and ejaculatory orgasms, underlining the complex nature of male sexual response and the need for further research to fully understand the spectrum of orgasmic experiences.
Limitations
The analysis explores the implications of this data, compares findings across studies, and investigates patterns in contraction characteristics between NEOs and maximal orgasms. However, it’s crucial to acknowledge the limitations of this analysis, including the small sample size and the lack of access to raw data. These constraints may impact the generalizability of the findings and highlight the need for more comprehensive research in this area. Limitations included that lack of clarity in the data from Bohlen et al. (1982), the low sample size, and the lack of published graphical data. I assumed that the participants were actually having the response participants claimed they had. The probes in the study were not tested across many studies for validation for accuracy. Different types of probes were also used. Artifacts, such as movement artifacts and interference by nearby muscle flexion could possibly change the contraction profile, such as making regular contractions irregular or a mix of regular and irregular contractions. Only Carmichael et al. also included the subjective length of perceived sensation of an orgasm to complement contraction data. Use of various probe sensors and different models of probes makes comparison in amplitudes difficult between studies.
Discussion
The anal contraction profiles in the literature during submaximal threshold response was compared to profiles during maximal threshold response. I hypothesized that the contractions in the NEO is different in frequency, amplitude, and duration than the maximal threshold refractory response. However, due to the limitations of the data and small sample size, no heuristic generalization can be definitively made. Therefore, I reject my hypothesis and revise, as the verdict is still out. The new hypotheses are as follows:
- As a submaximal threshold response, NEO contractions exist on a spectrum from no contractions to contractions that match or nearly match at least one feature (amplitude, frequency, and duration) of the range of contractions seen in maximal threshold refractory ejaculatory orgasms.
- One’s NEO contractions profile is most likely to resemble one’s contraction type(s) at PONR (regular, irregular, and a mix of both) identified by Bohlen et al. (1980).
Individual variation is common in many aspects of sexuality. It is not a surprise to find yet another possible individual variation in the study of submaximal threshold response. The spectrum of difference to sameness in the data analysis is not surprising given the individual variability in other reflexes. While not nearly as complex and multidimensional as the non-ejaculatory orgasm and orgasm at the PONR, other reflexes in the body can be complex and individually varied. For instance, “[d]eep tendon reflexes can be normal, absent, diminished, brisker, or asymmetrical, largely ranging in intensity from one person to another; in some rare cases they cannot be elicited even by using the best technique under normal conditions. Any asymmetry should be considered pathological, but it may be difficult to say if the abnormal reflex corresponds either to the side that seems brisker or to the side on which it seems diminished” (Pedroso, 2008, p. 11). It would make sense the both the NEO contractions and ejaculation both work with the orgasm/ejaculatory reflex, but with individual and threshold-specific factors for the features of the contraction. Research into hyperflexia and hyperflexia in other reflexes in the body notes variation in response ranging from hypereflexia to hyperreflexia (Walker, Hall, & Hurst, 1990). The convention for grading deep tendon reflexes are graded on a scale: 0 = no response; always abnormal; 1+ = a slight but definitely present response; may or may not be normal; 2+ = a brisk response; normal; 3+ = a very brisk response; may or may not be normal; and 4+ = a tap elicits a repeating reflex (clonus); always abnormal (Walker, Hall, & Hurst, 1990).
As a researcher, conceptualization of things called orgasm as well as extant orgasm typologies in the literature has been my focus. No typology exists for contractions that come with the NEO, as Bohlen et al. have done for the maximal threshold ejaculatory orgasm: Type 1 (a simple series of regular contractions), Type 2 (regular series and then irregular contractions), Type 3: (preliminary contractions before the series of regular contraction in midorgasm), and Type 4 (no contractions although orgasm was reported. Type 4 was only reported in their study on women (Bohlen et al., 1982). Based on reports from member of r/multiorgasmic and other groups, NEOs, or at least a submaximal threshold level response that share a high percentage of dimensions with similar intensities, can occur without contractions. Furthermore, the contraction profiles of the non-ejaculatory orgasm and the non-refractory ejaculatory orgasm, two objectively distinguishable submaximal threshold responses, might be unique from each other and vary between individuals.
Given that NEO contractions work with the same orgasm contraction reflex, I suspect them to have a similar Type 1 to 4 typology as well, perhaps with their own subtypological nuances. Typology by slope of peak contractions, and contraction variability over time can also be possible. However, it may be possible that they are all of the same type, although I do not think this is the case orgasmic instance and individual variability in preliminary data. I suspect that they are all distinguishable when taken into account the total spectrum of frequency and amplitude. Perhaps one might argue that something at least is different in the totality of the contractions given that they are not producing the full ejaculation. Perhaps NEO contractions are more likely to be of the same type as the one that the person has at full climax most often. Finally, some reports (including my own) of contractions of the penis and anus are out of sync with the orgasm, with the throbbing and contractions occurring a second or two after the 15-secondsdiscpr+ NEO sensation had faded. This has also occurred with non-refractory ejaculatory orgasms. Perhaps there are those that coincide with sensations and those that are discordant with other key dimensions and physiological correlates of orgasm, yield a discordant and non-discordant NEO typology. These as well of other potential contraction profiles are an opportunity for future research.
Conclusion and Future Research
Although no definitive conclusion was reached regarding whether submaximal threshold responses and maximal threshold responses have different or similar contraction profiles, this review of available contraction data has highlighted an under-explored area of male sexuality: submaximal orgasmic responses. The limited data available suggest possibilities beyond the traditional view of male sexuality, which often simplifies men’s sexual experiences to a single erogenous zone, the penis, with a singular response. This perception frequently leads to the dismissal of research on male pleasure, assuming that everything about it is already known. Contrary to this belief, male sexuality is complex, a term typically reserved for describing female sexuality (Gouvernet, Wunsch, & Brenot, 2019), with vast potential for full-body pleasure. While this paper focused on submaximal penile threshold responses, male sexuality encompasses various pleasure typologies that future research should address.
More research is needed to test the following new hypotheses:
- As a submaximal threshold response, NEO contractions exist on a spectrum from no contractions to contractions that match or nearly match at least one feature (amplitude, frequency, and duration) of the range of contractions seen in maximal threshold refractory ejaculatory orgasms.
- One’s NEO contractions profile is most likely to resemble one’s contraction type(s) at PONR (regular, irregular, and a mix of both) identified by Bohlen et al. (1980).
To facilitate such research, the development of accessible, low-cost, marketable smart anal probe technologies is essential. Open-source projects like Smart Ass Plug, which produce research-grade probe data, show promise. These projects use the silicone tubing design by Prause and Arnold (2019), inspired by Bohlen & Held (1979). An ideal product would be app-compatible, gender-neutral, accurate, and less prone to user artifacts. It should also be as scalable and marketable as the Lioness, yet far more affordable (e.g. less than $50).
Apart from technological barriers, several other challenges exist in studying submaximal threshold responses:
- Many clinicians, physicians, sex researchers, and sex educators are unaware of submaximal threshold responses in males and do not prioritize them in sexual function assessments.
- Funding typically focuses on solving problems rather than enhancing pleasure. There is no industry dedicated to submaximal threshold dysfunction—and there should not be medicalization of the NEO. Most research funding for male sexual health goes to efforts associated with the ejaculatory orgasm, fertility, and erectile function, leaving the study of other orgasmic responses in males neglected (Frith, 2015).
- The ability to experience multiple submaximal threshold responses in the population appears to be rare (Wibowo & Wassersug, 2016). Dunn and Trost (1989) describe males who have always had submaximal threshold level responses and those who have learned later in life. With clearer information and research into this topic, the submaximal threshold response might be more common. Given the dual control model and dynamic nature of the thresholds, one’s proclivity to learn to have submaximal threshold responses might correspond to interospective abilities, a sense of ejaculatory control, ability to relax, masturbation frequency, and several other factors that future researchers might identify.
- The notion that males cannot experience multiple peak responses without a refractory period makes any claim of male multiple penile orgasms seem dubious. Numerous self-help books claim to offer methods for achieving male multiple orgasms. A researcher might not wish to be associated with such authors.
Significant gaps in the literature present numerous research opportunities:
- Comparison of other contractile profiles (penile pulsation) during submaximal and maximal responses.
- Development of a new closeness to maximal threshold response scales. This psychometric can be used to correlate subjective rating of closeness to the contraction profile of the NEO. Contractions alone might not be enough to differentiate between responses, although it is a highly weighted correlate. Other dimensions and subjective report should also be considered. Despite the claim that one knows when they are having a response, that is not always the case. These can not only help the researcher but also the participant recognize what response they might be having.
- Exploration of whether one’s other reflexes correlate with contraction type during orgasm, especially the cremasteric reflex (testis retraction induced by stimulation of the skin on the front and inner thigh) and the superficial anal reflex (anal contraction induced by stimulation of anal skin).
- Determining how study of other reflexes can aid in the study of typology-by-contractions. Parameters considered by clinicians include threshold for stimulus, velocity of contraction, strength of contraction, duration of contraction, duration of relaxation phase, and response of other muscles that were not tested, and the overflow effect, which occurs when a reflex responds by testing nearby muscles) (Walker, Hall, & Hurst, 1990). Overactivity and weakness of muscles, the influence of relaxing versus tensing various muscles on the reflex, the influence of various movements on the reflex, and even the influence of psychological states and emotions on reflex attenuation and inhibition can influence reflex parameters and the ease that it occurs (Lang, Bradley, & Cuthbert, 1992). Each of these parameters could be used for orgasm-by-contraction typology.
- Assessment of submaximal threshold level response contractions with and without ejaculation. Considering the variability in contraction types during full orgasm and the possibility of 1 to 4 types of maximal climax (as suggested by Bohlen’s typology with a small sample and 1980s technology), future research should compare NEOs to the same participant’s full climax rather than to others’ or an average. Identifying types of full climax through a large sample of anal probe data, followed by at least 100 NEO sessions, could provide valuable insights.
- Inclusion of partner perceptions of contractions in future research. In a way, their body is like a sensor that can sense penile contractions. Similarly, a penetrating partner’s penis, neopenis, finger, or member is like a sensor for anal contractions.
- Assessment of whether anal, inguinal (via muffing), neovaginal contraction profiles during maximal and submaximal threshold responses.
- Do response priors change contraction profiles? That is, as more maximal threshold orgasms and NEOs are had, some changes might occur due orgasmic priors due to the difference in contraction type might not be as important of a dimension beyond a good correlate for orgasm. The type of contraction might not be that important of a factor considering all the factors of pleasure and orgasm. Another possibility is the tendency to have more ejaculatory-like contractions as time goes on due to the tendency towards the PONR over the session. It remains unknown whether ejaculatory or NEO priors can alter typology or later NEOs, especially during marathon sessions and many sessions throughout the day.
- Submaximal contraction profiles in females, those with anejaculation, spinal cord injury and paralysis, and post-op transgender males have yet to be explored in a dedicated study. Note that transgender women might prefer gender-confirming or gender neutral typologies, like Power’s (1992) plateau phase orgasm, rather than those for individuals who are cis and assigned male at birth.
- Do techniques influence contraction profiles? For example, do Kegels, a popular technique for NEOs, be more likely to cause a NEO contraction by helping to trigger the reflex, while relaxation-based approaches might be more associated with NEOs without contractions?
- Exploration of non-rhythmic and other contractions reported in forums such as r/prostateplay and the Aneros forum. An unexplored aspect is that the contraction reflex can be triggered far away from the PONR or out of sync with other sensations of orgasm, such as a couple seconds after NEO sensations. This suggests that the contractions are not essential for NEO sensations but sometimes coincide. Other types of contractions that are non-rhythmic are also reported in forums such as r/prostateplay and the Aneros forum. With enough Kegels, especially during the Aneros session, a flutter type contraction can be had in the anus with very low Arousal per PONR(t), not even having an erection. Several other contractions responses under orgasm-by-contraction typology have rectal profiles, such as when the clamps onto the dildo involuntarily or involuntarily pushes out. The typology and subtypology of such nonrhythmic contractions can be a topic of future study.
- Possible submaximal threshold responses in animal species. Calibrated vibration is a possible modality for such animal response given maximal threshold modelling (See Liu et al., 2017.).
- Given the possible evolutionary similarity, embryological development, and research showing similarities in the male and female maximal threshold climax, there may also be some similarities in contraction responses leading up to this maximal threshold for both males and females.
- An undocumented way NEO or NEO-like contractions occurs is part of my experience. When I am close to the PONR and have a powerful vibrator on the exterior of my anus. Instead of the orgasmic ejaculatory inevitability sensations that are usually most felt in the penis are felt in my anus with a burst of involuntary anal contractions which can occur back-to-back. I plan to produce data on this in the future.
Creating a research to-do list is much easier than actually conducting the study. Submaximal threshold level responses, such as the NEO (Non-Ejaculatory Orgasm), without contractions are particularly challenging to study objectively due to the lack of clear markers. Researchers often have to rely on subjective questionnaires, such as the Orgasm Rating Scale. NEOs without contractions can be similar to what Powers (1992) refers to as plateau phase orgasms in females, where a clitoral orgasm is reported without any contractions. Thus, studying submaximal responses in males is also relevant for females. This parallel makes sense given the byproduct hypothesis, the similarity in full penile and clitoral climaxes between sexes, and their common embryological development. NEOs with contractions are easier to study since contractions provide an objective marker distinguishing orgasm from non-orgasm. Insights from studying NEOs without contractions might be useful for understanding female submaximal threshold pleasures as well. Researchers will need to innovate and create novel methods for studying NEOs rather than relying on traditional approaches used for maximal threshold responses. This requires new models and interdisciplinary frameworks.
Future researchers should also consider the implications of non-mutual exclusivity of submaximal responses when assessing maximal response. Individuals with anorgasmia or difficulty reaching the maximal threshold might still experience pleasurable submaximal threshold responses. In studies on both male and female multiple orgasms, researchers need to distinguish between maximal and submaximal threshold responses. Prause found that many women who believe they are orgasming are not experiencing contractions (Covert, 2017; Weiss, 2018), suggesting a submaximal threshold response or another form of orgasm. In terms of a female zone theory, a subset of deemed multiorgasmic women, especially those reporting hundreds of orgasms, might be having numerous submaximal threshold responses (plateau phase responses) until they eventual reach full climax, which is described as a terminative orgasm or big, satisfying orgasm at the end of a series of responses. The other subset, likely a smaller percentage, is having several maximal orgasm responses close together. Emission typologies, such as male squirting, female squirting, female ejaculation, prostate milking, etc., are considered submaximal responses, and their arousalmetric will be model different than Arousal per PONR (t).No probe data exists to support claims of multiple maximum threshold response in the double or triple digits. This hypothesis can be a topic of future study. Similar to females in Prause’s study, a similar phenomenon may occur with NEOs in males, although all sampled studies of NEOs showed visible contractions.
Just like how some females might not recognize they are having an orgasm, many males labeled as “monoorgasmic” might actually experience several unnoticed submaximal threshold responses with or without contractions, as orgasm is often equated with ejaculation. If any submaximal threshold response is noted, it is typically the non-refractory ejaculatory orgasm due to the visible ejaculation (Kothari, 1989; Whipple, Myers, and Komisaruk, 1998). In most studies, contractions or a non-refractory ejaculatory must be present for it to be counted as an orgasm and the participant as “multiorgasmic.” While this may be controversial and might be seen as invalidating to males who call themselves “multiorgasmic,” the term “multiple submaximal threshold response” is more technical than “multiorgasmic,” as there is no universal definition of orgasm and debate exists about whether submaximal threshold responses qualify as orgasms. Nonetheless, one’s pleasure potential is not lessened any means by this specific terminology.
After reviewing the available literature, there is not enough evidence for any general conclusion. Like almost everything else in sexuality, the existing data suggest that there is some amount of individual variability. The question is whether this is in the normal range enough to say that they are basically the same, which will require much more data. If they are the same, it could pose a challenge for physiologists who will need to employ additional measures to differentiate maximal and submaximal threshold response. Perhaps an anal probe revolution driven by the next generation of curious researchers and new sex tech engineers could lead to a better understanding of submaximal and maximal threshold responses in their various contractile presentations and other dimensions.
References
Arnold, R. (2020). PLAY ME: interactive sonification of sexual arousal in long-distance relationships. Paladyn, Journal of Behavioral Robotics, 11(1), 250-270.
Arnold, R. (2020). PLAY ME: interactive sonification of sexual arousal in long-distance relationships. Paladyn, Journal of Behavioral Robotics, 11(1), 250-270.
Bergler, E. (1944). The problem of frigidity. The Psychiatric Quarterly, 18, 374–390
Blyuss, K, & Kyrychko, Y. (2023). Sex, ducks, and rock “n” roll: Mathematical model of sexual response. Chaos 1 April 2023; 33 (4): 043106.
Bohlen, J. G., & Held, J. P. (1979). An anal probe for monitoring vascular and muscular events during sexual response. Psychophysiology, 16(3), 318-323.
Bohlen, J. G., Held, J. P., & Sanderson, M. O. (1980). The male orgasm: pelvic contractions measured by anal probe. Archives of Sexual Behavior, 9(6), 503-521.
Bohlen/ J., Held/ J., Sanderson/ M., & Ahlgren, A. (1982a). The female orgasm: pelvic contractions. Archives of Sexual Behavior/ 11, 367-386.
Bohlen/ J./ Held/ J., Sanderson/ M./ & Boyer/ C. (1982b). Development of a woman’s multiple orgasm pattern: a research case report. The Journal of Sex Research/ 18/
Chia, M., & Abrams, D. (2009). The multi-orgasmic man: Sexual secrets every man should know. Harper Collins
Covert, J. (2017). Inside the Orgasm Lab. Retrieved from https://www.menshealth.com/sex-women/a18770869/female-orgasm-study-research/
Dunn, M.E., Trost, J.E. Male multiple orgasms: A descriptive study. Arch Sex Behav 18, 377–387 (1989). https://doi.org/10.1007/BF01541970
Fithian, M. & Hartman, W. (1984). Any man can: The multiple orgasmic technique for every loving man. Retrieved from https://www.amazon.com/Any-man-can-multiple-technique/dp/0312045204
Frith, H. (2015). Orgasmic bodies: The orgasm in contemporary western culture. Springer.
Frith, H. (2019). Visualising the ‘real’and the ‘fake’: Emotion work and the representation of orgasm in pornography and everyday sexual interactions. In Diversity in Gender and Visual Representation (pp. 4-16). Routledge.
Gérard, M., Berry, M., Shtarkshall, R. A., Amsel, R., & Binik, Y. M. (2021). Female Multiple Orgasm: An Exploratory Internet-Based Survey. Journal of sex research, 58(2), 206–221. https://doi.org/10.1080/00224499.2020.1743224
Gilmour, P. (2019). What is an orgasm? A neuroscientist explains what’s really going on when you climax. Retrieved from https://www.cosmopolitan.com/uk/love-sex/sex/a23864447/what-is-an-orgasm/#r3z-addoor
Gouvernet, B., Wunsch, S., & Brenot, P. (2019). L’orgasme masculin est-il complexe? Etude exploratoire des discours sur l’orgasme de 923 hommes en couple. Sexologies, 28(2), 73-82.
Hite, S. (1976). The Hite report. New York: Dell Publishing Co., Inc.
Hone Health. (2024). The Surprising Truth About Orgasms: The REAL Differences Between Women and Men. Retrieved from https://www.youtube.com/watch?v=xcaeJLV8unI
Janssen, E., & Bancroft, J. (2006). The dual control model: The role of sexual inhibition & excitation in sexual arousal and behavior. In E. Janssen (Ed.), The psychophysiology of sex (pp. 197–222). Indiana University Press.
Janssen, E., & Bancroft, J. (2023). The dual control model of sexual response: new findings and research directions. Sexologies, 32(2), 132-144.
Keesling, B. (1994). How to Make Love All Night (And Drive a Woman Wild : Male Multiple Orgasm and Other Secrets for Prolonged Lovemaking). Retrieved from https://www.amazon.com/Make-Love-Night-Drive-Woman/dp/0060171227
Kinsey, A. C., Pomeroy, W. B., Martin, C. E., & Gebhard, P. H. (1998). Sexual behavior in the human female. Indiana University Press.
Kline-Graber, G., & Graber, B. (1975). A guide to sexual satisfaction: woman’s orgasm. New York: Popular Library.
Kothari, P. (1989). Multiorgasm: Psychophysiodynamics. In P. Kothari (Ed.), Orgasm: New dimensions (pp. 103-127). Bombay, India: VRP Publishers
Kressbach, M. (2024). Sensing Health: Bodies, Data, and Digital Health Technologies. Ann Arbor: University of Michigan Press., https://doi.org/10.1353/book.119905.
Lang, P. J., Bradley, M. M., & Cuthbert, B. N. (1992). A Motivational Analysis of Emotion: Reflex-Cortex Connections. Psychological Science, 3(1), 44-49. https://doi.org/10.1111/j.1467-9280.1992.tb00255.x
Lee, A. (2019). Male Orgasms vs Female Orgasms: Is There a Difference? Retrieved from https://lioness.io/blogs/sex-guides/male-orgasm-versus-female-orgasm-is-there-a-difference
Lee, A. (2019). Male Orgasms vs Female Orgasms: Is There a Difference? Retrieved from https://lioness.io/blogs/sex-guides/male-orgasm-versus-female-orgasm-is-there-a-difference
Liu, X., Baloch, Z., Wang, G., Xue, S., Huang, Q., & Yang, S. (2018). High efficient and non-invasive collection of ejaculates from rats using penile vibratory stimulation. Theriogenology, 106, 192–197. https://doi.org/10.1016/j.theriogenology.2017.10.024
Mah, K., & Binik, Y. M. (2001). The nature of human orgasm: a critical review of major trends. Clinical psychology review, 21(6), 823-856.
Marie S. Carmichael; Valerie L. Warburton; Jean Dixen; Julian M. Davidson (1994). Relationships among cardiovascular, muscular, and oxytocin responses during human sexual activity., 23(1), 59–79. doi:10.1007/bf01541618
Marie S. Carmichael; Valerie L. Warburton; Jean Dixen; Julian M. Davidson (1994). Relationships among cardiovascular, muscular, and oxytocin responses during human sexual activity., 23(1), 59–79. doi:10.1007/bf01541618
Masters, W. H. & Johnson, V. E. (1966). Human Sexual Response. Toronto; New York: Bantam Books.
Nouveaux Plaisirs. (2021). The science of male orgasm. Retrieved from https://www.nouveauxplaisirs.fr/la-science-orgasme-masculin-2/42395
Nouveaux Plaisirs. (2021). The science of male orgasm. Retrieved from https://www.nouveauxplaisirs.fr/la-science-orgasme-masculin-2/42395
Pedroso, F. S. (2008). Reflexes. Encyclopedia of Infant and Early
Childhood Development, 1–13.
doi:10.1016/b978-0-12-816512-6.00133-6
Petersen, J. R. (1977). The extended male orgasm. Playboy.
Ploeger, D. (2011). Electrode. Retrieved from https://vimeo.com/38581381
Powers, L. V. (1992). Orgasm: A heuristic typology. The Union
Institute. Retrieved from https://www.proquest.com/openview/a944a51435da35ba4d20d28726c7e01d/1?cbl=18750&diss=y&pq-origsite=gscholar
Prause, Nicole & Arnold, Rudolf. (2019). Anal pneumatics: Tool for the verification of orgasm contractions across genders. Submitted for Publication.
Robbins, M. B., & Jensen, G. D. (1978). Multiple orgasm in males. Journal of Sex Research, 14(1), 21-26.
Robbins, Mina B.; Jensen, Gordon D. (1978). Multiple orgasm in males. The Journal of Sex Research, 14(1), 21–26. doi:10.1080/00224497809550989
Schnarch, D. M. (1991). Constructing the sexual crucible: An integration of sexual and marital therapy (Vol. 550). WW Norton & Company.
SHERFEY, M. J. (1972). The nature and evolution of female
sexuality. New York:RandomHouse, 1972.
Tannahill, R. (1980). Sex in history. New York: Stein and Day.
theelims. (n.d.). Smart Ass Plug. GitHub. Retrieved from https://github.com/theelims/SmartAssPlug
van Netten, J. J., Georgiadis, J. R., Nieuwenburg, A., & Kortekaas, R. (2008). 8–13 Hz fluctuations in rectal pressure are an objective marker of clitorally-induced orgasm in women. Archives of Sexual Behavior, 37, 279-285.
Walker, H. K., Hall, W.
D., & Hurst, J. W. (1990). Clinical methods: the history, physical, and
laboratory examinations
Weiss, S. (2018). Some People’s Orgasms Are Actually a Series of Short Ones. Vice. Retrieved from https://www.vice.com/en/article/7xqq4g/women-short-orgasms
Whipple, B., Myers, B. R., & Komisaruk, B. R. (1998). Male multiple ejaculatory orgasms: A case study. Journal of Sex Education and Therapy, 23(2), 157-162.
Wibowo, E., & Wassersug, R. J. (2016). Multiple orgasms in men—what we know so far. Sexual Medicine Reviews, 4(2), 136-148.eviews, 4(2), 136-148.

Leave a comment